 Submit an article
Submit an article
Search
- Page Path
- HOME > Search
Research Paper
- Development and evaluation of a health education program to enhance middle school students’ climate adaptation competencies: a nonequivalent control group pretest–posttest study in Korea
- Jiyu Hyun, Ju Hee Kim
- J Korean Acad Nurs 2026;56(2):179-189. Published online May 22, 2026
- DOI: https://doi.org/10.4040/jkan.25139
-
 Abstract
Abstract
 PDF
PDF ePub
ePub - Purpose
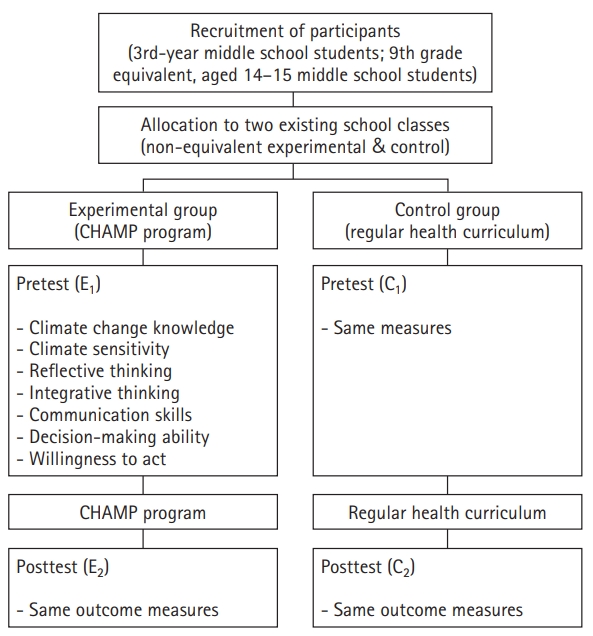
This study aimed to develop and evaluate the Climate and Health Action Mitigation Program (CHAMP), a health education intervention designed to enhance middle school students’ competencies for practicing climate adaptation behaviors in response to the health impacts of climate change.
Methods
A quasi-experimental pretest-posttest nonequivalent control group design was employed. Data were collected from October to December 2024. A total of 3rd-year middle school students; 9th grade equivalent, aged 14-15 students were assigned to either an experimental group that received the CHAMP intervention or a control group that received conventional health education. The CHAMP curriculum comprised six sessions developed using the ADDIE (Analysis, Design, Development, Implementation, and Evaluation) instructional design model and was aligned with the 2022 revised national health curriculum and the instructional hours stipulated in the School Health Act. Climate adaptation competency and its seven subdomains—climate-change knowledge, climate sensitivity, reflective thinking, integrative thinking, communication skills, decision-making ability, and willingness to act—were assessed before and after the intervention.
Results
Compared with the control group, the experimental group demonstrated statistically significant improvements (p<.01) in overall climate adaptation competency as well as in all seven subdomains. The largest improvements were observed in willingness to act, climate sensitivity, and climate-change knowledge. The CHAMP intervention was associated with meaningful improvements in students’ climate adaptation competencies, encompassing cognitive, behavioral, and attitudinal domains.
Conclusion
These findings support the feasibility and educational value of integrating climate–health content into the national curriculum. Future research should examine the scalability of CHAMP and evaluate its long-term sustainability and effects across diverse educational settings.
- 522 View
- 45 Download

Original Articles
- Study on Level of Anxiety on Admitted Patient's Family
- Hyun Sil Kim, Ju Hee Kim
- Journal of Nurses Academic Society 1983;13(1):42-56. Published online April 3, 2017
- DOI: https://doi.org/10.4040/jnas.1983.13.1.42
-
Abstract
PDF
The purpose of this study is to help the care of patient and to his family through comparison of the level of anxiety which between the family of admitted patient and the family without in patient, and to his family through comparison of the level of anxiety which between the family of admitted patient and the family without inpatient and exclude the factors which raised the level of anxiety in them. The experimental group in this study were samples of 200 patient's family selected by random sampling in H. University hospital located in Seoul (Department of patient were internal medicine, surgery, pediatrics and neuropsychiatry). The control group were samples of 70 family without inpatient selected by random sampling in Seoul. The data were collected through STAI (State-Trait Anxiety Inventory) by Spielberger (1970) for measurement to level of state and trait anxiety from April 1st to April 15th in 1982. The contents of data analysis by EDPS included the difference of level of anxiety between experimental and control group, correlationship between general characteristics of experimental group and level of anxiety, and correlation of trait and state anxiety in experimental group. The Findings of this study were as follows: 1) Level of anxiety of experimental group is higher than control group. 2) In the correlation between general characteristics and level of anxiety of experimental group, there were no significant difference which revealed in correlation with age of family member, family life cycle, marital status, the relation between patient and family member, the degree of symptom, number of admission, admission or nonadmission of medical insurance, number of family member, and division of disease to level of anxiety. However, according to the sex of family member, hospitallzation period, a monthly income of family, the degree of confidence toward medical team, religion of family, academic background of family, a tendency of significant differences to level of anxiety were seen. To put them in the concrete, they were as follow; a) Level of anxiety on female family member is higher than male in experimental group. fa) Admission period of patient is positively related to the level of anxiety of patient's family. c) The degree of confidence of patient's family toward medical team is in inverse proportion to the level of anxiety. d) A monthly income of patient's famly is in inverse proportion to the level of anxiety. e) Level of anxiety of believer in patient's family is lower than unbeliever, f) The academical background of patient's family is in inverse proportion to the level of anxiety. g) Level of state anxiety of patient's family at the time of admission is positively related to the evel of trait anxiety.
- 566 View
- 0 Download
- Study on the Determination of Nursing Hours by Self-Care Status of Patients
- Jung Sook Park, Ju Hee Kim
- Journal of Nurses Academic Society 1982;12(2):57-66. Published online April 3, 2017
- DOI: https://doi.org/10.4040/jnas.1982.12.2.57
-
Abstract
PDF
This Study was undertaken to delineate the relationship between numerical score and the amount of nursing hours required in the nursing process. Score was a numerical description of the patients functional nursing needs. Therefore this study focused on standard nursing hours required by patient's self-care status. This study observed the 62 patients and 15 R.N. in H. university hospital from Aug. 7, 1982 to Aug. 13, 1982. 1. For the first time, each head nurse assessed self-care status by Schoening's self-care score. Minimal care patient (self-care score: 23,24) was placed in Group I, intermediate care patient (self-care score: ll~22) was Group II, and special care score: 0~10) was Group III. 2. We observed and recorded the nursing care received from nurses according to patient's group. (8AM-4PM) 3. And, We observed and recorded the activities of nurses in order to determine standard nursing hours required. (8AM~4PM) 4. If we apply the content of paragraph 3 to paragraph 2, we will predict the number of patient that nurse can care during day time by self-care status. The following results were obtained: 1) Patieat's mean self-care score were Group 1 : 23.9 score Group 2 : 17.8 score Group 3 : 1.6 score 2) Nursipg hours required by patient's physical function (self-care status) status were Group 1 : 35 min. Group 2 : 47.5 min. Group 3 : 104. 6 min. 3) Nurse's nursing time and distribution required in nursing activities during day duty were A.D.L. : 84.3min. (17.56%) Functional nursing activities: 279.9min.(58.31%) Education & Emotional support: 11. 3min.(2.35%) Task unrelated patients : 54min.(11.25%) Non Productive nursing care : 50. 5min.(10. 52%) 4) Mean nursing hours required by each patient and the number of patient that nurse can care during day duty by self-care status were Group 1 : 38.6min. 11.1 patients/1 nurse Group 2 : 51. 1min. 8.4 patients/1 nurse Group 3 : 108.2min. 4 patients/1 nurse It seems reasonable that this could be done effectively as each-unit has an established standard for hours required. This not only allows time for planning of staff but helps to avoid the very human inelination to predict excessive staffing requirements by placing the majority of patients in high care group.
- 519 View
- 0 Download
- Testing the Validity and Reliability of FIPS(Face Interval Pain Scale) with Children's Pain from Intramuscular Injection
- Ju Hee Kim, Boon Han Kim
- Journal of Nurses Academic Society 1994;24(3):461-472. Published online March 31, 2017
- DOI: https://doi.org/10.4040/jnas.1994.24.3.461
-
Abstract
PDF
The main purpose of this study was to test the validity and reliability of FIPS as an assessment tool for pain in children. The subject were 81 children whose ages ranged from 3 to 14 years old who were experiencing pain from an intramuscular injection. 40 were being seen in a local primary hospital and 41 in a university hospital. The data were collected in two settings at a 6 month interval, the first was on Nov. 5th 1991 in a local clinic by one doctor, the second was on May 1st. 1992 in a university hospital by two nurse. McGrath's(1985) face interval cards and weight box scale which is a numeral scale that contains from one to five boxes of cards were used as measures. To analyze the subject's ability to use the face scale and weight box scale, statistical frequency was employed. To determine the difference in the rated pain intensity on the face interval scale and the weight box, Pearson correlation coefficent and t-test were employed. To compare the difference in the rated pain intensity of the face interval scale and the weight box scale according to subject's general characteristics, X2-test was employed. The findings were as follows; 1. The subject's ages were from 3 to 14 with a mean age of 8.3 years old. There were 54(66.7%) male children and 27(33.3%) female children. 2. The number of subjects who correctly displayed cards ranging from none to severe pain was 66(81. 5%) and the number who correctly compared two cards 3 times was 73 (90.1 %). 3. Correlation coefficents between each level card of the FIPS and WBS(Weight Box Scale) were r= .52~.80 P<0.01. 4. There was no statistical difference in rating of the intensity on the FIPS and WBS.(t=1.12~1.02, P<0.22~ 0.45). 5. The differences in rating pain intensity according to the children's general characteristics were related to age (X2 =8.94, P<0.05), but not to sex (X2=0.23, P=0.80).
- 496 View
- 1 Download
- Testing the Reliability of the Pain Color Circle Measurement Tool
- Ju Hee Kim
- Journal of Nurses Academic Society 1991;21(3):339-348. Published online March 31, 2017
- DOI: https://doi.org/10.4040/jnas.1991.21.3.339
-
Abstract
PDF
The study problem was to determine the reliability of the Stewart pain circle measurement tool with Korean subjects. The purpose was to assess the tool for potential use in research in Korea. The subjects were 95 primary school students and 103 university students in Seoul. The study was conducted from May to June 1990, using Stewart's pain color circle tool. To determine the difference in the rated intensity of the order of the pain circles, statistical mean and standard deviation were employed. Item reliability and test-retest reliability were used to explore for reliability. ANOVA and t-test were used to explore for differences in the rated intensity of the order of the pain color circles according to the subjects' general characteristics. The findings were as follows ; 1. Higher level pain intensity was assigned to color circle numbers 2, 4, and 6(These contain large amounts of color). Lower level pain intensity was assigned to numbers 1, 3, and 5(These contain small amounts of color). Higher and lower levels of pain intensity selection patterns were the same as Stewart's but the highest rating of pain was different. The highest pain intensity rating was given to the color red in this study instead of black as in Stewart's test. 2. University students and primary school students' ratings were not very different. 3. Pain color circle reliability was alpha=0.3468, Test-retest reliability was supported (t=0.02~0.97, p=0.337~0.988). 4. Differences in the rating of the pain intensity order were related to the subjects' age and sex, but not to religion. It was concluded tat the pain color circle measurement tool is worth for further study as a research instrument with both Korean adult and child clients for validity and reliability.
- 569 View
- 0 Download
- A Study for Testing Validity of Korean Pain Measurement Tool
- Ju Hee Kim
- Journal of Nurses Academic Society 1986;16(1):81-88. Published online March 31, 2017
- DOI: https://doi.org/10.4040/jnas.1986.16.1.81
-
Abstract
PDF
The main purpose of this study was to clarify the validity with patient's general background of Korean Pain Measurement tool. The subjects of this study were 195 patient from the 8 Med-Surgical wards in H. University Hospital in Seoul. The study was conducted over a 40 day period from Oct. 5, 1985 to Nov. 15, 1985. All patients had pain. Korean Pain Measurement tool and simple descriptive pain scale as Graphic Rating Scale were used to measure the pain. The Pearson Correlation Coefficient test was exercised to measure the correlation between the two kinds of pain tools. To clarify the Sensitivity of Korean Pain tool was used frequency with patient's response. To compare the diffenence in pain levels with patient's general background, ANOVA and t-test was employed. To compare the difference in pain levels existed due to pain area of the body used mean numbers. The outcome of the study was as follows: 1. A positive correlation did exist between two pain measurement tools.(r=.2028~. 7768, p<0.002) 2. The sensitive subclass in Korean Pain Measurement tools was 7 subclass. The 7 subclass are inflammatory repeated pain, simple stimulating, traction pressure, dull pain, cavity pain, digestion related pain, suffering-related pain. 3. The existence of levels of pain in accordance with patient's general background, the department of hospital, pain area of the body and school age was supported. Age, sex, religion, marrital status, economic status, acute or chronic status was not supported. 4. The existence of higher pain levels of the body area was anus, chest, and lower pain levels of the body area was eye, ear, nose and throat. Based on the above results, it was found that sensitive subclasses of the Korean Pain Measurement tool was 7 subclass among all of 20 subclass. Thus it can be concluded that Korean Pain Measurement tool when partialy used and supplemented, can be an effective tool of pain measurement for the patient in Korea.
- 548 View
- 3 Download
- A Descriptive Study on Pain of Elderly
- Ju Hee Kim, Kyung Hee Yang, Hyun Ju Lee
- Journal of Nurses Academic Society 1996;26(4):878-888. Published online March 30, 2017
- DOI: https://doi.org/10.4040/jnas.1996.26.4.878
-
Abstract
PDF
The main purpose of this study was getting related to the pain charactristic data of elderly. It contains past and present health status, daily living activity level, pain frequency, causes, pain area, pain intensity, pain worse causes, and pain releave causes, pain management methods. The subject were 79 elderly whose age were over 65 years old. They were lived in their home environment. Half of them were resident of middle range city at province and the others were Seoul city. The data was collected from Dec. 1st. 1995 to Jan. 30th. 1996. Interviews were held with semi-structured questionaire after pilot study by researchers. Pain measurement tool were used graphic rating scale and Abstract of Korean Pain Language Scale. To analize the subject's general characteristics, past and present health status, daily living activity level, characteristics about pain, pain management methods statistical SPSS for win frequency were employed. The findings were as follows; 1. There were 33(41.8%) male and 46(58.2%) female Below 69 year old were 20(25.3%), 70-79 year old were 42 (53.2%), over 80 year old were 17(21.5%), mean age was 74(from 65 to 89). 2. Buddhist were 24(30.4%), Christian were 29(36. 7%), the other religious status or nun religians were 26(32.9%). 3. Past good health status were 63(79.7%), not so good status were 6(7.6%). Present good health status were 19 (24.1%), moderated health status were 6(7.6%), not so good status were 14(17.7%). 4. Daily living activity limitation were 39(49.4%), nonlimitation of activity were 5(6.3%). 5. Walking limitation were 3(3.8%), nonlimitation walking were 52(65.8%). 6. Insomnia was 23(29.1%), no difficult were 38(48. 1%). 7. Chronic pain complaints were 64(81%), diseases causes of pain were 25(31.6%), bad health behavior causes of pain were 27(34.2%). 8. Most pain area were back 30(29.4%), leg 17(16. 7%), knee 16(15.7%), arm 13(12.7%), teeth, chest and head were each 5(4.9%), loin, trunk were each 4(3.9%), the other areas were 3(3%). 9. Pain intensity was 3.49(mean) by Korean Language Scale, 6.59(mean) by graphic rating scale. Sensitive pain was 3.5(47.9%), affective pain was 3(20.8%) It was high pain level and sensitive pain. 10. Most pain worse causes moving was 35(44.3%), pain relieving causes rest was 29(36.7%). 11. Pain management method were medication 40 (42.1%), physiotherapy 23(24.2%), hospital 12 (12.6%), the others 7(7.4%), none 13(13.7%). The conclusion; Present health status of eldery was not so good. Almost half of them have some diseases. Most common diseases of eldery were arthristis, respitatory and heart problems. Fourty nine percent of elderly had limitation of daily living activities. Eighty one percent of eldely had chronic pain. Most of them was back pain (30%). Pain intensity was high (score over 3.5). The worsening pain causes was moving and releiving causes was rest. Pain management method were pain medication, physiotherapy. Therefore, Nursing care plan for the elderly have to focus on pain because majority of elderly have chronic high level of pain related to the arthritis.
- 614 View
- 1 Download
- A Study on Attitude of Ethical Dilemmas in Clinical Nurses
- Ju Hee Kim, Soo Yeon Ahn, Ji Yoon Kim, Ju Yeon Chung, Ji Mee Kim, Sun Ha Choi, Young Eun Kwon, Mi Young Chon, Myoung Hee Kim
- Journal of Nurses Academic Society 1995;25(3):496-509. Published online March 30, 2017
- DOI: https://doi.org/10.4040/jnas.1995.25.3.496
-
Abstract
PDF
This study was conducted to identify the attitude of ethical dilemmas in hospital nurses. Ethical dilemmas were categorized into four areas: human life area, clients area, nursing practice area, and nurses-co-worker area. 354 nurses working in clinical settings were selected in Seoul and Kangwon area. Data were gathered from 26, June to 10, July, 1994 by structured guestionnaires. Descriptive statistics were employed to analyze the data. The results obtained from data were as follows: 1) In human life area mean score was 3.03. This area showed remarkabale individual differences between utilitarian and deonto-logical position. 2) In clients area mean score was 3.94. It means that nurses tend to take a deonto-logical position. 3) In nursing practice area mean score was 3.41. It means that nurses tend to take a slightly deontological position. 4) In nurses-co-worker area mean score was 3. It means that nurses tend to take a deont-ological position. To conclude, clinents area, nursing practice area, and nurses-co-worker area taken deontological position. Most nurse's primary concern was the 'welfare of the patients' which is to fundamental ethical professional practice. But nurses experienced more ethical dilemmas in human life area than others. Therefore, nurses should be prepared to make independent decision that based on bio-ethics and professional ethics.
-
Citations
Citations to this article as recorded by
- Case Development on Nurses' Ethical Dilemmas with Physicians' and Nurses' Decision Making
Jeong-Mee Jeong, Jung-Hyun Park, Seok Hee Jeong
Journal of Korean Academy of Nursing Administration.2013; 19(5): 668. CrossRef
- Case Development on Nurses' Ethical Dilemmas with Physicians' and Nurses' Decision Making
- 1,004 View
- 2 Download
- 1 Crossref
- The Concept Analysis of Ego-integrity in the Elderly
- Sung Ok Chang, Eun Sook Kong, Kwuy Bun Kim, Nam Cho Kim, Ju Hee Kim, Chun Gill Kim, Hee Kyung Kim, Mi Soon Song, Soo Yeon Ahn, Kyung Ja Lee, Young Whee Lee, Si Ja Chon, Nam Ok Cho, Myung Ok Cho, Kyung Sook Choi
- Journal of Korean Academy of Nursing 2004;34(7):1172-1183. Published online March 28, 2017
- DOI: https://doi.org/10.4040/jkan.2004.34.7.1172
-
Abstract
PDF
Purpose Ego-integrity in Erikson's stage theory is used frequently among health team members related to the care of the elderly and has specific meanings within the context of quality of life in later life. However, the concept of ego-integrity in the elderly has not been well articulated in the literature. This study was conducted clarify and conceptualize the phenomena of ego-integrity in the elderly.
Method A Hybrid Model of concept development was applied to develop a concept of ego-integrity, which included a field study carried out in Seoul, South Korea using in-depth interviews with old adults who were admitted as a right person for research subject according to attributes of ego-integrity analysed in the theoretical phase.
Results The concept of ego-integrity emerged as a complex phenomenon having meanings in several different dimensions which encompassed several attributes.
Conclusions Ego-integrity is a concept having needs that should be treated in a specific way and it is possible to enrich the meaning and methods to manage ego-integrity in nursing interventions for promoting quality of life so that its application may have effects that have positive impacts on the elderly's well being.
-
Citations
Citations to this article as recorded by- Smartphone proficiency and use, loneliness, and ego integrity: an examination of older adult smartphone users in South Korea
Kisun Kim, Sung-Yeon Park, Hyung-Cheol Kang
Behaviour & Information Technology.2021; 40(7): 625. CrossRef - Consideration of the Psychological and Mental Health of the Elderly during COVID-19: A Theoretical Review
Kunho Lee, Goo-Churl Jeong, JongEun Yim
International Journal of Environmental Research and Public Health.2020; 17(21): 8098. CrossRef - Ego-Integrity Management of Residents in Nursing Homes: A Concept Analysis based on the Method by Walker and Avant
Sun Young Lim, Sung Ok Chang
Journal of Korean Gerontological Nursing.2018; 20(2): 97. CrossRef - Relations between Gratitude Disposition and Ego-Integrity of Korean Elderly Men and Women: Mediating Effects of Generativity and Relatedness
Myeong Ae Choe, Jeong Shin An
Family and Environment Research.2017; 55(2): 181. CrossRef - The Influencing Factors on the Ego Integrity of Elderly Living Alone
Hyun Jeong Jeong, Sook Hee Yoon
The Journal of Korean Academic Society of Nursing Education.2015; 21(4): 499. CrossRef - Influence of Age-Identity on Existential Identity and Psychological Well-Being of the Elderly
Shin Sook Lee
Family and Environment Research.2014; 52(2): 151. CrossRef - Study on Knowledge of the Elderly's Physical, Psychological and Social Aspects among College Students in Physical Therapy
Chung-Joa Ahn, Myung-Chul Kim, Seung-Kyun Kim, Seul-Ki Han
Journal of the Korean Society of Physical Medicine.2014; 9(4): 375. CrossRef
- Smartphone proficiency and use, loneliness, and ego integrity: an examination of older adult smartphone users in South Korea
- 1,417 View
- 37 Download
- 7 Crossref
- Comparison of Cognitive Levels, Nutritional Status, Depression in the Elderly according to Living Situations
- Young Mi Jung, Ju Hee Kim
- Journal of Korean Academy of Nursing 2004;34(3):495-503. Published online March 28, 2017
- DOI: https://doi.org/10.4040/jkan.2004.34.3.495
-
Abstract
PDF
Purpose The purpose of this study was to compare the degree of cognitive level, nutritional status and depression in elderly according to living situations.
Method The subjects consisted of 173 elderly classifying three groups(living alone, living with spouse, living with children). Data was collected from March to June, 2003 by a structured questionnaire that included general characteristics, MMSE-K, nutritional status and depression scale. The collected data was analyzed by the SPSS program including descriptive statistics, χ2-test, ANCOVA, Scheffe test and Pearson Correlation Coefficient.
Result In MMSE-K, the living alone group showed suspicious dementia while the other groups were normal. The living alone group showed a high nutritional risk and all three groups showed depression. In MMSE-K, the nutritional status and depression were statistically significant by the living situation. In each group except living with spouse, MMSE-K indicated a significantly negative correlation to depression and nutritional status, while nutritional status showed a significantly positive correlation to depression.
Conclusion It is necessary to develop supportive programs for decreasing the risk of bad health in the elderly and an individual approach according to their living situation. Especially, more concern and intervention is necessary for the solitary elderly.
-
Citations
Citations to this article as recorded by- Effect of Home-Visit Cognitive Function Training Among National Long-Term Care Insurance Beneficiaries With Dementia in Korea
Sung Ok Han, Hyunjong Song
Journal of Gerontological Nursing.2026; 52(4): 55. CrossRef - A Study on the Status of Nutrition Management and Life Satisfaction among Elderly Living Alone in Korea.
Joo-Eun Lee
Current Research in Nutrition and Food Science Journal.2025; 13(2): 876-. CrossRef - Development of a frailty prevention program including nutrition and exercise interventions for older adults in senior daycare centers in South Korea using a mixed methods research design
Jiwon Sim, Jongguk Lim, Eunji Ko, Eunjin Jang, Minjeong Jeong, Sohyun Park
Nutrition Research and Practice.2024; 18(3): 372. CrossRef - Malnutrition Risk in Community-Dwelling Older Adults with Dual Sensory Declines: Focusing on Social Determinants of Health
Ha Na Jeong
Research in Community and Public Health Nursing.2024; 35: 325. CrossRef - The longitudinal reciprocal relationship between food insecurity and depressive symptoms among Korean elderly who live in poverty: application of auto-regressive cross-lagged model
Jayoung Cho
Asia Pacific Journal of Social Work and Development.2023; 33(2): 86. CrossRef - 고령자의 신체건강 및 식생활 행태가 영양소 섭취량에 미치는 영향
하리 임, 다솔 김, 나미 주
Korean Journal of Food and Cookery Science.2023; 39(6): 518. CrossRef - Factors influencing dementia prevention behaviors in older Koreans enrolled in senior welfare centers
Kyung-Choon Lim, Myoungsuk Kim, Hana Ko
The Journal of Korean Academic Society of Nursing Education.2021; 27(1): 39. CrossRef - Correlation between Sleep, Depression, Metabolic Syndrome and Cognition in Community Dwelling Elderly
Joohee Shim, Jihyun Baek
Journal of Health Informatics and Statistics.2021; 46(2): 212. CrossRef - Efficacy of Smart Speaker–Based Metamemory Training in Older Adults: Case-Control Cohort Study
Jeongsim Kim, EunJi Shin, KyungHwa Han, Soowon Park, Jung Hae Youn, Guixiang Jin, Jun-Young Lee
Journal of Medical Internet Research.2021; 23(2): e20177. CrossRef - Nutritional Risk of the Elderly Receiving a Home-Delivered Meal Service Program and the Factors for Nutritional Risk
Na-Young Yi, Jung-Hwa Choi
Korean Journal of Community Nutrition.2019; 24(3): 197. CrossRef - How Much Do Older Adults Living Alone in Rural South Korea Know About Dementia?
Mi Sook Kim, Dong-Soo Shin, Yong-jun Choi, Jin Soon Kim
Journal of Preventive Medicine and Public Health.2018; 51(4): 188. CrossRef - Association between physical health status, health behaviors and subjective depression among single-person household
Myung Sun Lee, Hyunjong Song, Boyoung Kim
Korean Journal of Health Education and Promotion.2018; 35(2): 61. CrossRef - Women's Health Status Working at Traditional Marketplaces and Their Needs for Public Health Care Services
Won Ju Hwang, Jin Ah Kim, Hee-Gerl Kim
Journal of Korean Academy of Community Health Nursing.2017; 28(1): 44. CrossRef - Key Food Selection for Assessement of Oral Health Related Quality of Life among Some Korean Elderly
Soo-Jeong Hwang
Journal of dental hygiene science.2016; 16(5): 361. CrossRef - Relationship between Sense of Belonging, Powerlessness and Nutritional status of Elderly People
Mi-Hye Kim, Hae-Kyung Chung
Journal of The Korean Society of Food Culture.2015; 30(1): 118. CrossRef - Nutrition States and Related Factors of Female Elderly according to Residence
Mi-Yeon Park
Journal of the East Asian Society of Dietary Life.2015; 25(1): 39. CrossRef - Nutritional Risk, Stress, and Health related Quality of Life among Older Women with a Foreign Daughter-in-Law
Mikyung Park, Kiwol Sung
Journal of Korean Public Health Nursing.2015; 29(2): 312. CrossRef - Effect on Cognitive Function in Elderly People
Jeong-Sook Lee, Sun-Young Lee
The Korean Journal of Health Service Management.2015; 9(3): 201. CrossRef - Structural and Associational Solidarity Between Adult Children and Older Parents: Impact on Older Parents' Cognitive Functioning
Heejeong Choi, Joohong Min
Journal of Korean Home Management Association.2015; 33(4): 105. CrossRef - A study on dietary habits and food intakes in adults aged 50 or older according to depression status
Seungjae Lee, Yuri Kim, Sunhee Seo, Mi Sook Cho
Journal of Nutrition and Health.2014; 47(1): 67. CrossRef - Elderly Health and Literature Therapy: A Theoretical Review
Yeongcheol Eum, Jongeun Yim, Wonjae Choi
The Tohoku Journal of Experimental Medicine.2014; 232(2): 79. CrossRef - Comparison of Demographic Characteristics, Comorbidity, and Health Habits of Older Adults with Mild Cognitive Impairment and Older Adults with Normal Cognitive Function
Myonghwa Park, Mi Ra Sung, Sun Kyung Kim, Dong Young Lee
Journal of Korean Academy of Nursing.2014; 44(4): 351. CrossRef - The Relationships among Satisfaction with Food-Related Life, Depression, Isolation, Social Support, and Overall Satisfaction of Life in Elderly South Koreans
Sunhee Seo, Misook Cho, Yuri Kim, Jiyoon Ahn
Journal of the Korean Dietetic Association.2013; 19(2): 159. CrossRef - Effects of a Cognition Activation Program for the Institutionalized Old-Old in Korea
Hung Sa Lee, Dohyun Lee
Journal of Korean Academy of Community Health Nursing.2013; 24(4): 427. CrossRef - Depression and Suicidal Ideation in Elders with Dementia
Jong Pil Kim, Mi-Yeul Hyun
Journal of Korean Academy of Nursing.2013; 43(2): 296. CrossRef - Influence of Malnutrition and Social Network on Health-related Quality of Life in Elders
Hee Kyung Kim, Hae Kyung Chang, Mi-Ra Lee, Youn-Jung Son, Su Jeong Han, Nam Young Yang, Myoung-Ran Yoo, Seon Young Choi, Youn Mi Kim
Journal of Korean Academy of Fundamentals of Nursing.2013; 20(2): 98. CrossRef - Different Influence of Risk Factors on Self-rated Health between The Economically Poor and Non-poor Elderly Populations Living Alone: Based on One Sub-area in Seoul
Young-Mi Ko, Youngtae Cho
Korean Journal of Health Education and Promotion.2013; 30(2): 41. CrossRef - Nutritional Risk, Perceived Health Status, and Depression of the Young-Old and the Old-Old in Low-Income Elderly Women
Myung-Suk Lee
Journal of agricultural medicine and community health.2012; 37(1): 12. CrossRef - Gender Difference in Risk Factors for Depression in Community-dwelling Elders
Chul-Gyu Kim, Seungmi Park
Journal of Korean Academy of Nursing.2012; 42(1): 136. CrossRef - Prevalence and Correlates of Depression in Older Koreans: Comparison of Young-old and Old-old
Kyung-Choon Lim, Seonho Kim
Journal of Korean Academy of Psychiatric and Mental Health Nursing.2012; 21(1): 1. CrossRef - Relations among Depression, Life Satisfaction and Health Promoting Behavior in the Elderly
Ji-Hye Seo, Hyun-Sook Ryu
Journal of Korean Academy of Community Health Nursing.2010; 21(2): 169. CrossRef - The Relationship of Perceived Health Status, Activities of Daily Living and Nutrition Status in the Community-Dwelling Korean Elderly
Younhee Kang, Miyoung Kim, Eliza Lee
Journal of Korean Academy of Nursing.2008; 38(1): 122. CrossRef
- Effect of Home-Visit Cognitive Function Training Among National Long-Term Care Insurance Beneficiaries With Dementia in Korea
- 1,314 View
- 15 Download
- 32 Crossref
- Health Promoting Behavior in Pregnant Couples: Actor-Partner Interdependence Model Analysis
- Ju Hee Kim, Young-A Song
- J Korean Acad Nurs 2017;47(4):467-475. Published online January 15, 2017
- DOI: https://doi.org/10.4040/jkan.2017.47.4.467
-
Abstract
PDF
Abstract Purpose This study aimed to identify the actor and partner effects of self-efficacy, marital adjustment, and social support on the health promoting behavior of Korean pregnant couples.
Methods Participants were 132 couples who met the eligibility criteria. Data were collected from June to November, 2016 at a community health center. The Actor-Partner Interdependence Model was used for analyzing the actor and partner effects of self-efficacy, marital adjustment, and social support on health promoting behavior.
Results The fitness indices for the model were GFI=0.90, NFI=0.92, CFI=0.91, TLI=0.90, and RMSEA=0.04, which satisfied the criteria. Self-efficacy had actor and partner effect on health promoting behavior of wives, but had only actor effect of on health promoting behavior of husbands. Marital adjustment showed actor and partner effect on the health promoting behavior of pregnant couples. Social support only had an actor effect on the health promoting behavior of wives. And, marital adjustment and social support had a mutual effect.
Conclusion This study indicates that the partner involvement is needed to develop health promotion programs for pregnant couples.
-
Citations
Citations to this article as recorded by- Health‐Promoting Behaviour Patterns in Women With Gestational Diabetes Mellitus: A Latent Class Analysis and Association With Prenatal Depression
Zhang Jiayuan, Luo Xiaoxi, Chen Dan, Zhou Yuqiu
Journal of Clinical Nursing.2026; 35(1): 133. CrossRef - The Effects of Maternal-Fetal Attachment, Pregnancy Stress, and Social Support on Prenatal Health Care Behavior in Pregnant Women
Heeji Jeon, Seonho Kim
Journal of Korean Maternal and Child Health.2026; 30(2): 103. CrossRef - Factors Influencing Health-Promoting Behaviors Among Primigravidas of Advanced Maternal Age
Jeongeun Lee, Hyunkyung Choi
Journal of Korean Maternal and Child Health.2026; 30(2): 91. CrossRef - Serial mediation effects of social support and antepartum depression on the relationship between fetal attachment and anxiety in high-risk pregnant couples of South Korea
Mihyeon Park, Sukhee Ahn
Journal of Korean Academy of Nursing.2025; 55(1): 19. CrossRef - Associations between behavior cognition–social influence and pregnancy planning behavior in China: An integrated individual-couple analysis
Ruyu Sun, Tingzhong Yang, Menmen Wang, Xinxin Ying, Lu Li, Weifang Zhang
Preventive Medicine.2025; 199: 108363. CrossRef - Factors associated with clinical nurses’ preconception health behavior in Korea: a cross-sectional survey
Yoon-Jung Park, Sun-Hee Kim
Women's Health Nursing.2024; 30(1): 79. CrossRef
- Health‐Promoting Behaviour Patterns in Women With Gestational Diabetes Mellitus: A Latent Class Analysis and Association With Prenatal Depression
- 1,703 View
- 34 Download
- 6 Crossref
- Effect of Music Intervention on Maternal Anxiety and Fetal Heart Rate Pattern During Non-Stress Test
- Myung Ok Oh, Young Jeoum Kim, Cho Hee Baek, Ju Hee Kim, No Mi Park, Mi Jeong Yu, Han Sol Song
- J Korean Acad Nurs 2016;46(3):315-326. Published online June 30, 2016
- DOI: https://doi.org/10.4040/jkan.2016.46.3.315
-
Abstract
PDF
Purpose The purpose of this cross-over experimental study was to examine effects of music intervention on maternal anxiety, fetal heart rate pattern and testing time during non-stress tests (NST) for antenatal fetal assessment.
Methods Sixty pregnant women within 28 to 40 gestational weeks were randomly assigned to either the experimental group (n=30) or control group (n=30). Music intervention was provided to pregnant women in the experimental group during NST. Degree of maternal anxiety and fetal heart rate pattern were our primary outcomes. State-trait anxiety inventory, blood pressure, pulse rate, and changes in peripheral skin temperature were assessed to determine the degree of maternal anxiety. Baseline fetal heart rate, frequency of acceleration in fetal heart rate, fetal movement test and testing time for reactive NST were assessed to measure the fetal heart rate pattern.
Results The experimental group showed significantly lower scores in state anxiety than the control group. There were no significant differences in systolic blood pressure and pulse rate between the two groups. Baseline fetal heart rate was significantly lower in the experimental group than in the control group. Frequency of acceleration in fetal heart rate was significantly increased in the experimental group compared to the control group. There were no significant differences in fetal movement and testing time for reactive NST between the two groups.
Conclusion Present results suggest that music intervention could be an effective nursing intervention for alel viating anxiety during non-stress test.
-
Citations
Citations to this article as recorded by- The effect of spousal support during the non-stress test on the anxiety levels of pregnant women and fetal well-being: a randomized controlled study
Yeter Şener, Mürüvvet Başer
Advances in Mental Health.2025; 23(3): 335. CrossRef - The effect of virtual reality on pregnant women and fetuses: a systematic review and meta-analysis of randomized controlled trials
Xiaopu Shi, Chunguang Liang, Haitao Ren, Chunxia Liao, Na Yue
Archives of Gynecology and Obstetrics.2025; 312(2): 337. CrossRef - The effects of the pregnant woman’s mental visualization of her baby during the non-stress test on maternal anxiety and fetal parameters: A randomized controlled clinical trial
Fatma Keskin Töre, Cansu Ağralı, Gülçin Nacar, Özlem Özel Özcan
Advances in Integrative Medicine.2025; 12(4): 100508. CrossRef - The effect of virtual reality on fetal movement, fetal heart rate, maternal satisfaction, fatigue, and anxiety levels and vital signs of pregnant women during non-stress test: A randomized controlled trial
Eylem Toker, Mine Gökduman Keleş
Health Care for Women International.2024; 45(7): 765. CrossRef - The effects of listening to lullabies and self-selected music at home on prenatal stress and anxiety in nulliparous pregnant women: A randomized-controlled study
Nazlı Baltacı, Özlem Doğan Yüksekol, Emine Koç, Mihriban Ulucan
Health Care for Women International.2024; 45(5): 562. CrossRef - Fetuses can Listen, Learn, and Remember: We Need to be Cautious about What and How We Say It!
Akhil Maheshwari, Thierry AGM Huisman, Srijan Singh, Gayatri Athalye-Jape, Adrianna Frydrysiak-Brzozowska, Kedar Jape, Kinga Piórkowska
Newborn.2024; 3(4): 281. CrossRef - The effect of virtual reality and music on anxiety, non-stress test parameters, and satisfaction of high-risk pregnant women undergoing non-stress tests: Randomized controlled trial
Neslihan Yılmaz Sezer, Menekşe Nazlı Aker, Aykan Yücel, Dilan Çalışıcı
European Journal of Obstetrics & Gynecology and Reproductive Biology.2024; 296: 52. CrossRef - Effect of Virtual Reality and Music Therapy on the Physiologic Parameters of Pregnant Women and Fetuses and on Anxiety Levels: A Randomized Controlled Trial
Fatima Estrella‐Juarez, Mar Requena‐Mullor, Jessica Garcia‐Gonzalez, Antonia Lopez‐Villen, Raquel Alarcon‐Rodriguez
Journal of Midwifery & Women's Health.2023; 68(1): 35. CrossRef - Effectiveness of Music on Perinatal Anxiety Among Pregnant Women and Newborn Behaviors: A Systematic Review and Narrative Synthesis
Meena Konsam, Sonia R. B. D’Souza, Samir Kumar Praharaj, Baby S. Nayak, Jyothi Shetty, Shashikala Bhat, Judith A. Noronha, Sunita Panda
Indian Journal of Psychological Medicine.2023; 45(6): 565. CrossRef - Effects of music therapy on the fetal outcomes of non-stress test and maternal anxiety
L. Fathi, A. Shakarami, K. Amraei, F. Yari, A. Behzadvand
Neuropsychiatrie de l'Enfance et de l'Adolescence.2023; 71(6): 316. CrossRef - Environmental factors influencing women’s childbirth experiences in labor–delivery–recovery–postpartum unit: a qualitative cross-sectional study
Ashraf Kazemi, Marjan Beigi, Hajar Enteshary Najafabadi
BMC Pregnancy and Childbirth.2023;[Epub] CrossRef - The effect of music on fetal well-being and anxiety levels and vital signs of pregnant women during non-stress test: Turkey sample
Nurseli Soylu, Tülay Bülbül, İptisam İpek Müderris
Health Care for Women International.2022; 43(5): 499. CrossRef - Renkli Abdominal Örtü ve Kemer Kullanımının Non-Stress Test Parametreleri ve Maternal Kaygıya Etkisi: Randomize Kontrollü Bir Çalışma
Esra GÜNEY, Zeynep BAL, Esra KARATAŞ OKYAY, Tuba UÇAR
Samsun Sağlık Bilimleri Dergisi.2022; 7(2): 393. CrossRef - The Effect of a Breathing Relaxation Therapy for Pregnant Women with Preterm Labor Pain: a Systematic Review and Meta-Analysis
Seo-A Park
Keimyung Medical Journal.2021; 40(1): 39. CrossRef - Interventions among Pregnant Women in the Field of Music Therapy: A Systematic Review
Bruna Mayumi Omori Shimada, Magda da Silva Oliveira Menezes dos Santos, Mayara Alvares Cabral, Vanessa Oliveira Silva, Gislaine Cristina Vagetti
Revista Brasileira de Ginecologia e Obstetrícia / RBGO Gynecology and Obstetrics.2021; 43(05): 403. CrossRef - The effectiveness of music on the result of non-stress test
Tuan Vo, Anh Huynh, Thao Nguyen Thi Thu, Lora Claywell
MedPharmRes.2020; 4(3): 12. CrossRef - The Effect of Music on Fetus Movement During Non-Stress Test
Batoul Khodakarami, Marzieh Janesari Ladani, Farideh Kazemi, Soudabeh Aghababaei
Avicenna Journal of Nursing and Midwifery Care.2020; 28(4): 1. CrossRef - The effect of music on the non-stress test and maternal anxiety
Hatice Erkun Dolker, Fatma Basar
Complementary Therapies in Clinical Practice.2019; 35: 259. CrossRef - Müziğin non-stres test üzerine etkilerinin incelenmesi
Ramazan DENİZLİ, Nayif ÇİÇEKLİ, Gökhan GÜLYAŞAR, Yasmin ABOALHASAN, Taylan AYGÜN, Nihat FARİSOĞULLARI, Önder SAKİN
SDÜ Tıp Fakültesi Dergisi.2019; 26(4): 464. CrossRef - The effect of music on the results of a non-stress test: A non-randomized controlled clinical trial
Didem Şimşek Küçükkelepçe, Sermin Timur Taşhan
European Journal of Integrative Medicine.2018; 18: 8. CrossRef - The effect of traditional Persian music on the cardiac functioning of young Iranian women
Behzad Abedi, Ataollah Abbasi, Atefeh Goshvarpour, Hamid Tayebi Khosroshai, Elnaz Javanshir
Indian Heart Journal.2017; 69(4): 491. CrossRef
- The effect of spousal support during the non-stress test on the anxiety levels of pregnant women and fetal well-being: a randomized controlled study
- 3,096 View
- 74 Download
- 21 Crossref
- A Structural Model for Quality of Life of Infertile Women
- Ju Hee Kim, Hye Sook Shin
- J Korean Acad Nurs 2013;43(3):312-320. Published online June 28, 2013
- DOI: https://doi.org/10.4040/jkan.2013.43.3.312
-
Abstract
PDF
Purpose The purpose of this study was to test a model for quality of life among infertile women. This model was based primarily on the concept of the Fertility Quality of Life by Boivin et al. (2011) and the Infertility Resilience Model by Rindenour (2009).
Methods Fifteen measurable variables were used to estimate quality of life. They included endogenous variables such as fertility quality of life and resilience, and exogenous variables such as infertility related stress, depression, marital adjustment, and family support. Data sets (n=203) used for analysis were collected in a general hospital which had, on average, 400 assisted reproductive technologies per month.
Results The assessment of the modified model indicated acceptable fit, with χ2/d.f=2.07, GFI=.90, AGFI=.89, NFI=.89, CFI=.91, RMSEA=.07. Depression, infertility related stress, marital adjustment, resilience, and family support had direct influences on quality of life.
Conclusion The results of this study should contribute to the development of nursing intervention programs to enhance quality of life using factors that affect fertiQol (fertility quality of life) of infertile women.
-
Citations
Citations to this article as recorded by- The mediating effect of health-promoting behaviors on the relationship between infertility stress and fertility-related quality of life of infertile women: a cross-sectional study
Eun Jin Kim, Ju-Hee Nho, Hye Young Kim
Women's Health Nursing.2025; 31(1): 66. CrossRef - The effects of a lifestyle intervention for men in infertile couples in South Korea: a non-randomized controlled trial
Yun Mi Kim, Ju-Hee Nho
Journal of Korean Academy of Nursing.2025; 55(2): 191. CrossRef - Effectiveness of a couple-based mobile programme in improving human fertility
Soo Kyoung Hann, Hee Sun Kang, Ju Hee Kim
Journal of Reproductive and Infant Psychology.2025; : 1. CrossRef - A Scoping Review of the Effect of the COVID-19 Pandemic on Patients Under Infertility Treatment
Boyoung Jeon, Hongbi Kim, Hye In Jeong
Journal of The Korean Society of Maternal and Child Health.2023; 27(2): 80. CrossRef - Quality of Infertility Care Services and Emotional Health of South Asian Women
Sehar-un-Nisa Hassan, Aqeela Zahra, Nuzhat Parveen, Naveed Iqbal, Sarwat Mumtaz, Asma Batool
Psychology Research and Behavior Management.2022; Volume 15: 1131. CrossRef - The Reliability and Validity of Korean Version of the Infertility Stigma Scale (K-ISS)
Miok Kim, Minkyung Ban
Journal of Korean Academy of Nursing.2022; 52(6): 582. CrossRef - The Mediating Role of Self-esteem between Spousal Support and Infertility-related Stress among Infertile Couples: Actor Effects and Partner Effects
Ka Yeon Lee, Seong Hee Kim
Family and Environment Research.2021; 59(4): 465. CrossRef - Associations of Symptoms of Depression, Social Support, and Quality of Life Among Korean Women Who Experience Infertility
Hyewon Shin, Jungmin Lee, Shin-Jeong Kim, Minjeong Jo
Journal of Obstetric, Gynecologic & Neonatal Nursing.2021; 50(6): e1. CrossRef - Predictive Model for the Quality of Life of Infertile Men
Jummi Park, Nayeon Shin
The Open Nursing Journal.2021; 15(1): 9. CrossRef - The Study of Relationship among Infertility Stress, Gratitude, and Couple Relationship Changes of Women Undergoing Reproductive Treatments
Miok Kim, Jummi Park, Ju-Eun Hong, Minkyung Ban
Journal of The Korean Society of Maternal and Child Health.2021; 25(3): 169. CrossRef - Effects of Mind–Body Programs on Infertile Women: A Systematic Review and Meta-analysis of Randomized Controlled Trials
Ju-Young Ha, Seon-Hwa Ban
Asian Nursing Research.2021; 15(2): 77. CrossRef - A moderated mediation model of perceived stress, negative emotions and mindfulness on fertility quality of life in women with recurrent pregnancy loss
Guopeng Li, Zhenhua Jiang, Xue Han, Xue Shang, Wanli Tian, Xiaofei Kang, Mei Fang
Quality of Life Research.2020; 29(7): 1775. CrossRef - Factors influencing infertility-related quality of life in infertile women
Yun Mi Kim, Ju-Hee Nho
Korean Journal of Women Health Nursing.2020; 26(1): 49. CrossRef - Effects of psychological intervention for Korean infertile women under In Vitro Fertilization on infertility stress, depression, intimacy, sexual satisfaction and fatigue
Miok Kim, So-Hyun Moon, Jee-Ean Kim
Archives of Psychiatric Nursing.2020; 34(4): 211. CrossRef - Effects of uncertainty and spousal support on infertility-related quality of life in women undergoing assisted reproductive technologies
Hye Shin Lee, Sunjoo Boo, Jeong-Ah Ahn, Ju-Eun Song
Korean Journal of Women Health Nursing.2020; 26(1): 72. CrossRef - Effect of resilience on infertile couples’ quality of life: an actor–partner interdependence model approach
Ju-Young Ha, Seon-Hwa Ban
Health and Quality of Life Outcomes.2020;[Epub] CrossRef - Nursing needs assessment scale for women with infertility: development and validation
Jummi Park, Nayeon Shin, Kyungmi Lee
Korean Journal of Women Health Nursing.2020; 26(2): 141. CrossRef - Effects of Irrational Parenthood Cognition, Family Support, and Resilience on Depression of Infertile Women
Eun Young Cho, Mi-Hae Sung
Korean Journal of Women Health Nursing.2019; 25(1): 60. CrossRef - Factors Affecting the Infertility-Related Quality of Life among the Infertility Women
Young Hee Lee, Jung Suk Park
Journal of The Korean Society of Maternal and Child Health.2019; 23(3): 191. CrossRef - A Dyadic Approach to Infertility Stress, Marital Adjustment, and Depression on Quality of Life in Infertile Couples
Ju Hee Kim, Hye Sook Shin, Eun Kyoung Yun
Journal of Holistic Nursing.2018; 36(1): 6. CrossRef - Factors Influencing Infertility-related Quality of Life in Women Undergoing Assisted Reproductive Techniques: Focusing on Depression and Resilience
You Jung Jung, Hye Young Kim
Korean Journal of Women Health Nursing.2017; 23(2): 117. CrossRef - Effects of Irrational Parenthood Cognition, Post Traumatic Stress Disorder and Spousal Support on Quality of Life of Infertile Women
So Ra Yang, Jung Hee Yeo
Korean Journal of Women Health Nursing.2017; 23(2): 145. CrossRef - Psychometric Properties of the Korean Version of the Infertility Self-Efficacy Scale
Ju Hee Kim, Han Jong Park, Jung Ho Kim, Soojin Chung, Hyon Joo Hong
Asian Nursing Research.2017; 11(3): 159. CrossRef - A Phenomenological Study on the Spontaneous Abortion Experiences of Women
Ju-Eun Hong, Jum-Mi Park
Korean Journal of Women Health Nursing.2017; 23(2): 63. CrossRef - Screening for infertility‐related stress at the time of initial infertility consultation: psychometric properties of a brief measure
Giulia Casu, Paola Gremigni
Journal of Advanced Nursing.2016; 72(3): 693. CrossRef - The Mediating Effect of Resilience on Depression and Rehabilitation Motivation in Stroke Patients
Eun Sil Choi, Eun Nam Lee, Jeong Lim Cho
Journal of muscle and joint health.2016; 23(1): 19. CrossRef - Infertility Stress, Depression, and Resilience in Women with Infertility treatments
Miok Kim, Hyuna Nam, Misun Youn
Journal of Korean Public Health Nursing.2016; 30(1): 93. CrossRef - Factors Influencing the Depression Level of Couples Participating in the National Supporting Program for Infertile Couples
Nami Hwang, Insun Jang
Journal of Korean Academy of Community Health Nursing.2015; 26(3): 179. CrossRef
- The mediating effect of health-promoting behaviors on the relationship between infertility stress and fertility-related quality of life of infertile women: a cross-sectional study
- 1,971 View
- 23 Download
- 28 Crossref
- Impact of Prepregnancy Body Mass Index on Pregnancy Outcome in Women with a Singleton Conceived by Assisted Reproductive Technology and Spontaneously Conceived Pregnancy: A Case-Control Study
- Ju Hee Kim, Hye Sook Shin, Bo Kyung Park, Kwang Moon Yang, Young Ho Lee, Hyun Mee Ryu
- J Korean Acad Nurs 2012;42(4):517-524. Published online August 12, 2012
- DOI: https://doi.org/10.4040/jkan.2012.42.4.517
-
Abstract
PDF
Abstract Purpose To compare and confirm the impact of prepregnancy body mass index on pregnancy outcome in women with a singleton conceived by assisted reproductive technology and spontaneously conceived pregnancy.
Methods A sample of 165 and 247 pregnant women with and without assisted reproductive technology were retrospectively recruited from electronic medical charts of C hospital.
Results There were significant differences between the two groups for maternal age, paternal age, length of marriage, prepregnancy body mass index, parity, spontaneous abortion experience, and preterm delivery. A prepregnancy body mass index of ≥25 was associated with higher risk for maternal and neonatal complication in the assisted reproductive technology group.
Conclusion The results indicate that a higher prepregnancy body mass index is associated with increased risks for adverse pregnancy outcomes for women using assisted reproductive technology. So these women need appropriate care to compensate for the risk.
- 871 View
- 0 Download
- Development of a Scale to Measure Korean Ego-integrity in Older Adults
- Sung Ok Chang, Eun Sook Kong, Kwuy Bun Kim, Nam Cho Kim, Ju Hee Kim, Chun Gill Kim, Hee Kyung Kim, Mi Soon Song, Soo Yeon Ahn, Kyung Ja Lee, Young Whee Lee, Si Ja Chon, Nam Ok Cho, Myung Ok Cho, Kyung Sook Choi
- Journal of Korean Academy of Nursing 2007;37(3):334-342. Published online April 30, 2007
- DOI: https://doi.org/10.4040/jkan.2007.37.3.334
-
Abstract
PDF
Purpose Ego-integrity in older adults is the central concept related to quality of life in later life. Therefore, for effective interventions to enhance the quality of later life, a scale to measure ego-integrity in older adults is necessary. This study was carried out to develop a scale to measure ego-integrity in older adults.
Methods This study utilized cronbach's alpha in analyzing the reliability of the collected data and expert group, and factor analysis and item analysis to analyze validity.
Results Seventeen items were selected from a total of 21 items. Cronbach's alpha coefficient for internal consistency was .88 for the 17 items of ego-integrity in the older adults scale. Three factors evolved by factor analysis, which explained 50.71% of the total variance.
Conclusion The scale for measuring ego-integrity in Korean older adults in this study was evaluated as a tool with a high degree of reliability and validity.
-
Citations
Citations to this article as recorded by- The Association Between Depression and Death Anxiety Among Older Adults: Moderating Effect of Ego-Integrity
Jin-Hee Woo, Sung-Man Bae
OMEGA - Journal of Death and Dying.2025; 90(3): 1025. CrossRef - The effects of ego integrity and readiness for death on the preferences of care near the end-of-life of hospitalized older adults in long-term care hospitals: A cross-sectional correlation study
Jangmi Baek, Jun-Ah Song
Journal of Korean Gerontological Nursing.2023; 25(2): 185. CrossRef - Development of Assessment Tool for Ego-Integrity in Nursing Home Residents
Sun Young Lim, Sung Ok Chang
Journal of Korean Gerontological Nursing.2020; 22(2): 140. CrossRef - Factors Influencing Death Anxiety in Community-Dwelling Elderly: Based on the Ecology Theory
Yeonha Kim, Minju Kim
The Korean Journal of Hospice and Palliative Care.2019; 22(1): 30. CrossRef - Ego-Integrity Management of Residents in Nursing Homes: A Concept Analysis based on the Method by Walker and Avant
Sun Young Lim, Sung Ok Chang
Journal of Korean Gerontological Nursing.2018; 20(2): 97. CrossRef - The Influencing Factors on the Ego Integrity of Elderly Living Alone
Hyun Jeong Jeong, Sook Hee Yoon
The Journal of Korean Academic Society of Nursing Education.2015; 21(4): 499. CrossRef - Mutual Reciprocal Relationship between Ego Integrity and Depression in Elderly: Multi-dimensional Influencing Factors
Hye Sun Jeong, Hyun Soo Oh
Korean Journal of Adult Nursing.2015; 27(3): 262. CrossRef - Exploring Wisdom in the Korean Elderly: A Q Methodology Study
Kiwol Sung
Asian Nursing Research.2011; 5(2): 128. CrossRef - Korean Older Adults' Perceptions of the Aging Process
Yeon-Gang Chung, Kyung-Hee Kim, Kyung-Sook Choi, Hye-Jin Kwon, Kyung-Sook Park, Mi-Hye Choi, Young-Hee Yom
Journal of Gerontological Nursing.2008; 34(5): 36. CrossRef
- The Association Between Depression and Death Anxiety Among Older Adults: Moderating Effect of Ego-Integrity
- 1,486 View
- 39 Download
- 9 Crossref
 First
First Prev
Prev

