 Submit an article
Submit an article
Articles
- Page Path
- HOME > J Korean Acad Nurs > Volume 54(3); 2024 > Article
- Research Paper Effects of a Pre-Conception Care Program in Women with Inflammatory Bowel Disease: A Mixed-Methods Study Including a Randomized Controlled Trial
- Young Jin Lee, Hae Won Kim, Yeon Hee Kim, Suk-Kyun Yang, Ji-Yeon Kim
-
Journal of Korean Academy of Nursing 2024;54(3):386-402.
DOI: https://doi.org/10.4040/jkan.24010
Published online: August 31, 2024
1College of Nursing, Eulji University, Uijeongbu, Korea
2College of Nursing, Seoul National University, Seoul, Korea
3Center for World-leading Human-care Nurse Leaders for the Future by Brain Korea 21 (BK 21) Four Project, College of Nursing, Seoul National University, Seoul, Korea
4The Research Institute of Nursing Science, College of Nursing, Seoul National University, Seoul, Korea
5Department of Clinical Nursing, University of Ulsan, Seoul, Korea
6Department of Gastroenterology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
2College of Nursing, Seoul National University, Seoul, Korea
3Center for World-leading Human-care Nurse Leaders for the Future by Brain Korea 21 (BK 21) Four Project, College of Nursing, Seoul National University, Seoul, Korea
4The Research Institute of Nursing Science, College of Nursing, Seoul National University, Seoul, Korea
5Department of Clinical Nursing, University of Ulsan, Seoul, Korea
6Department of Gastroenterology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
-
Corresponding author:
Suk-Kyun Yang,
Email: haewon@snu.ac.kr
Abstract
Purpose
The purpose of this study was to conduct a pre-conception care program for women of childbearing age with inflammatory bowel disease (IBD) in Korea and verify its effects on self-efficacy for IBD management, IBD-related pregnancy knowledge, and IBD-related pregnancy anxiety. It also aimed to explore the changes in participants through the program.
Methods
A convergent mixed-methods study design was adopted. In the quantitative phase, 35 women (17 and 18 in the intervention and control group, respectively) participated. The intervention group attended a program that included small-group sessions and individual tele-coaching. To confirm the effects, data were collected before and one and four weeks after the intervention. In the qualitative stage, focus group interviews and tele-coaching were conducted with the intervention group.
Results
After the program ended, significant differences were observed over time between the intervention and control groups for self-efficacy for IBD management (Wald χ2 = 4.41, p = .036), IBD-related pregnancy knowledge (Wald χ2 = 13.80, p < .001) and IBD-related pregnancy anxiety (Wald χ2 = 8.61, p = .003). Qualitative data analysis revealed the following themes: (1) improving confidence in IBD management and awareness for planned pregnancy; (2) improving IBD awareness related to pregnancy and childbirth; and (3) relieving anxiety about and actively facing pregnancy.
Conclusion
This study is meaningful in that, to the best of our knowledge, it is the first to develop a pre-conception care program for women diagnosed with IBD and confirm its effectiveness. Furthermore, this program is expected to be suitable for patient counseling and education in clinical practice.
J Korean Acad Nurs. 2024 Aug;54(3):386-402. English.
Published online Aug 31, 2024.
https://doi.org/10.4040/jkan.24010
Published online Aug 31, 2024.
https://doi.org/10.4040/jkan.24010
© 2024 Korean Society of Nursing Science
Original Article
Effects of a Pre-Conception Care Program in Women with Inflammatory Bowel Disease: A Mixed-Methods Study Including a Randomized Controlled Trial
Abstract
Purpose
The purpose of this study was to conduct a pre-conception care program for women of childbearing age with inflammatory bowel disease (IBD) in Korea and verify its effects on self-efficacy for IBD management, IBD-related pregnancy knowledge, and IBD-related pregnancy anxiety. It also aimed to explore the changes in participants through the program.
Methods
A convergent mixed-methods study design was adopted. In the quantitative phase, 35 women (17 and 18 in the intervention and control group, respectively) participated. The intervention group attended a program that included small-group sessions and individual tele-coaching. To confirm the effects, data were collected before and one and four weeks after the intervention. In the qualitative stage, focus group interviews and tele-coaching were conducted with the intervention group.
Results
After the program ended, significant differences were observed over time between the intervention and control groups for self-efficacy for IBD management (Wald χ2 = 4.41, p = .036), IBD-related pregnancy knowledge (Wald χ2 = 13.80, p < .001) and IBD-related pregnancy anxiety (Wald χ2 = 8.61, p = .003). Qualitative data analysis revealed the following themes: (1) improving confidence in IBD management and awareness for planned pregnancy; (2) improving IBD awareness related to pregnancy and childbirth; and (3) relieving anxiety about and actively facing pregnancy.
Conclusion
This study is meaningful in that, to the best of our knowledge, it is the first to develop a pre-conception care program for women diagnosed with IBD and confirm its effectiveness. Furthermore, this program is expected to be suitable for patient counseling and education in clinical practice.
Keywords
Anxiety; Inflammatory Bowel Diseases; Knowledge; Preconception Care; Self Efficacy
INTRODUCTION
Inflammatory bowel disease (IBD), which includes Crohn’s disease (CD) and ulcerative colitis (UC), is a disease that causes inflammation in the gastrointestinal tract. IBD is a chronic disease with no cure, that requires continuous symptom management, as recurrence is common [1, 2]. Recently, the number of IBD patients in Korea has increased rapidly, and interest in the disease is also increasing. According to a study analyzing the IBD incidence rate in Korea over 30 years, from 1986 to 2015; in 1986~1990, the IBD incidence rate stood at 0.35 per 100,000 inhabitants, whereas in 2011~2015, it surged to 8.26 per 100,000 inhabitants [2]. This rapid increase in prevalence is noteworthy because it has been found to be most prominent among countries in East Asia [2].
In particular, IBD mainly occurs in young age groups, so it is important for women with IBD to have healthy pregnancies and childbirth. Women with IBD had higher risks of preterm birth, low birth weight, stillbirth, and congenital anomalies than healthy women [3]. In a study investigating the birth outcomes of women diagnosed with IBD in Korea over the past 10 years, women diagnosed with CD had higher rates of caesarean sections, stillbirths, and intrauterine growth restriction than healthy women. Preterm birth was more common in women diagnosed with UC [4]. However, these negative birth outcomes in women with IBD are related to disease activity during pregnancy, not to the disease itself [4, 5]. Women with IBD who are in remission have similar fertility rates and pregnancy outcomes to those of healthy women. However, when disease activity is high at conception, the rate of negative birth outcomes is higher than it is for women in remission [4]. Therefore, women of childbearing age who are capable of becoming pregnant or who are preparing for pregnancy should manage their disease after sufficient consultation with medical professionals to maintain a remission period before conception [4, 5].
Almost all women with IBD who had never been pregnant recognized that the disease could harm pregnancy and believed that pregnancy would make the disease worse [6, 7]. A recent study targeting women with IBD confirmed that most IBD drugs, including amino-salicylate, biological agents, and thiopurine, except methotrexate, are safe for women preparing for pregnancy, during pregnancy, and after childbirth [8, 9, 10]. Therefore, it is emphasized that women who are planning to become pregnant should continue taking their IBD medications to maintain the IBD remission phase. Nonetheless, women with IBD tend to voluntarily stop taking drugs to treat IBD during pregnancy due to the mistaken belief that those all drugs can harm the fetus, and they have concerns about heredity and fear of giving birth to a child with a deformity due to disease or drugs [8, 11]. Such IBD-related pregnancy anxiety may lead to voluntary childlessness [7, 11].
Anxiety and negative beliefs concerning pregnancy among women with IBD are deeply rooted in a lack of knowledge [7], and women with IBD in Korea tend to have low levels of knowledge about pregnancy [11, 12]. Therefore, accurate information about pregnancy should be provided to women with IBD to reduce their anxiety and help them consider pregnancy. It is already known that it is important for women with IBD to maintain remission during pregnancy, but so far, study related to pregnancy has only focused on the knowledge, anxiety, and outcomes of pregnancy in women with IBD. The effects of a pre-conception program for women with IBD to maintain remission for a healthy pregnancy have yet to be examined.
To promote better health management behaviors for maintaining remission, self-efficacy (the ability to manage one’s health independently) is required [13]. A high degree of self-efficacy corresponds to positive health-related behaviors and attitudes, as well as improved stress management. As a resource for enhancing self-efficacy, Bandura [14] described performance accomplishment, which refers to actually performing the behavior, the vicarious experience obtained through the successful behavior of others in a similar situation, verbal persuasion, and the physiological state. Previous studies have already proven the effectiveness of education developed using self-efficacy enhancement resources to improve the self-management ability of patients diagnosed with IBD [13, 15]. Despite the importance of maintaining remission period prior to pregnancy for women with IBD preparing for pregnancy, there has not been a program developed to improve their health care self-efficacy. Therefore, in this study, a self-efficacy improvement strategy was applied to develop and apply a pre-conception program and evaluate its effectiveness. This study was conducted to evaluate whether a pre-conception care program for women with IBD (PCCP-IBD) based on self-efficacy theory is effective in improving self-efficacy related to IBD management, which is the primary outcome of this study. In addition, we examined the improvements in IBD-related pregnancy knowledge and the reduction of IBD-related pregnancy anxiety (secondary outcome). A qualitative study was also conducted to gain a deeper understanding of the changes experienced by participants through the program.
The hypotheses of this study were as follows: First, there will be a significant difference in self-efficacy for IBD management scores between the intervention group and the control group. Second, there will be a significant difference in IBD-related pregnancy knowledge score and IBD-related pregnancy anxiety score between the intervention group and the control group.
METHODS
1. Study design
This study employed a convergent mixed-methods design to analyze quantitative data from a randomized controlled pre-posttest design and qualitative data from focus group interviews and tele-coaching to test the effectiveness of the PCCP-IBD [16]. The quantitative data of the program were collected through a randomized controlled pre-posttest design, and the qualitative data were collected through two focus group interviews and individual interviews through tele-coaching. The study design for the quantitative study is shown in Figure 1.
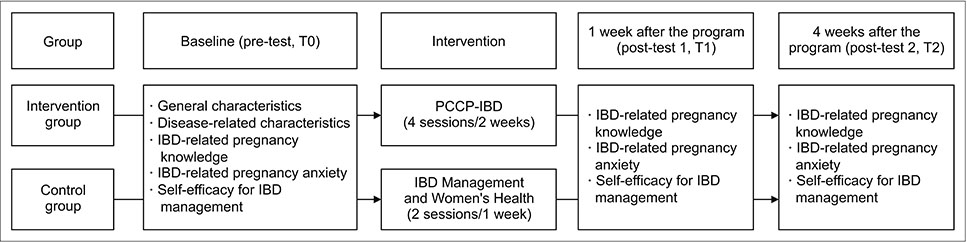
Figure 1
Design of the quantative study.
IBD = Inflammatory bowel disease; PCCP-IBD = Pre-conception care program for women with inflammatory bowel disease.
A randomized controlled trial was conducted from February to April 2020 following the Consolidated Standards of Reporting Trials recommendations and flow charts [17]. This randomized controlled trial was conducted with one intervention group and one control group. This was a single-blind study, and it was not known until the end of the study whether the participants were in the intervention or control group.
2. Participants
Those eligible to participate in this study were adult women aged 20~45 years who had been diagnosed with CD or UC with no previous childbirth experience and who understood the purpose of the study and voluntarily agreed to take part. Women who were scheduled for surgery or hospitalization were excluded from the study to avoid any potential impact of a relapse of their disease status on their anxiety or self-efficacy.
The sample size for conducting quantitative study was calculated using G*power version 3.1 [18]. Due to the lack of previous studies related to this study, the medium effect (f = .25) was set as the effect size required for repeated measures ANOVA. The result of calculating the significance level at .05 and the statistical power at .80 was 28 participants. When recruiting participants, we recruited 46 people, considering that there would be a large number of dropouts due to the outbreak of coronavirus disease 2019 (COVID-19) and changes in the participants’ disease status. The number of participants for conducting qualitative study was all 17 people in the intervention group for quantitative study who wished to participate in the interview.
The participants were recruited from a tertiary hospital located in Seoul by placing posters and leaflets with recruitment information at the IBD center and online through a survey platform. Initially, 48 women volunteered to participate in the program, but two withdrew due to the COVID-19 pandemic and trips. A sample of 46 participants meeting the participant selection criteria was numbered and randomized using the case random sampling process in IBM SPSS Statistics 25 (IBM Co.). After inputting the ratio of the intervention group and the control group at 1:1, 23 participants were assigned to each group. Participants were randomly assigned to the intervention or control groups. However, after the participants allocation was completed, 11 women withdrew their participation due to social distancing in Korea related to the COVID-19 pandemic, personal schedules, and changes in their health conditions. Finally, 17 women in the intervention group and 18 women in the control group participated in this study. After providing program to the intervention group and control group, one person in the intervention group did not respond to the survey for unknown reasons after one week of the intervention, and one person did not respond to the survey for unknown reasons from the survey after four weeks. Finally, 17 participants in the intervention group responded to the final survey and 18 participants in the control group responded to the survey four weeks after the intervention (Figure 2).

Figure 2
Process of the study based on the CONSORT flow diagram.
COVID-19 = Coronavirus disease 2019.
Measurements
1) Inflammatory bowel disease self-efficacy scale (IBD-SES)
This questionnaire developed by Keefer et al. [19] was used to measure self-efficacy for IBD management. This questionnaire has 29 items across four sub-areas: managing stress and emotions, managing medical care, managing symptoms and the disease, and maintaining remission. Each item is scored on a 10-point Likert scale, with possible scores ranging from a minimum of 29 to a maximum of 290. A higher score indicates a higher degree of self-efficacy. The questionnaire was translated into Korean according to the World Health Organization (WHO)’s [20] tool translation and application guidelines. First, after obtaining approval to use the questionnaire from the original author, it was translated into Korean by a researcher who is fluent in English and Korean and has research experience in translating English instruments. Afterwards, a nursing researcher who was not familiar with the original questionnaire back-translated it from Korean into English. The original questionnaire and the back-translated questionnaire were sent to a professional translator for verification and completion. The questionnaire translated into Korean was verified for content validity by eight experts, including a nursing professor and a gastroenterologist. The content validity index (CVI) was .89 to 1.00 following validation by eight experts. Cronbach’s alpha in this study was .97.
2) The Crohn’s and colitis pregnancy knowledge
The Crohn’s and colitis pregnancy knowledge questionnaire was used to measure IBD-related pregnancy knowledge. Approval for use of the questionnaire was obtained from the original author and the Korean translator. This scale developed by Selinger et al. [12] and translated into Korean by Lee et al. [11] was used to measure participants’ IBD-related pregnancy knowledge. This widely-used tool contains 17 multiple-choice items. Each item is worth 1 point if it is correct and 0 points if it is incorrect, with a minimum of 0 points and a maximum of 17 points. A total score of 0 to 7 is considered ‘poor,’ 8 to 10 is considered ‘adequate,’ 11 to 13 is considered ‘good,’ and 14 or higher is considered ‘very good.’ Kuder–Richardson 20 was .83 in this study.
3) The IBD-specific reproductive concerns questionnaire
To measure IBD-related pregnancy anxiety, the IBD-specific reproductive concerns questionnaire developed by Huang [21] was translated into Korean and modified by the researcher for this study. Approval was obtained from the original authors for the translation of the questionnaire and its utilization in this study. The questionnaire was translated into Korean in accordance with the WHO’s [20] tool translation and application guidelines by one researcher who is fluent in English and Korean and has experience conducting research on English tool translation. Afterwards, a nursing researcher who was not familiar with the original questionnaire back-translated the Korean back into English. The original questionnaire and the back-translated questionnaire were sent to a professional translator for verification and then completed. Four items were deleted from the original set of 14 items because they were deemed unrelated to this study through a research meeting, leaving eight items in final. The revised questionnaire was verified for content validity by eight experts, including a nursing professor and a gastroenterologist. The CVI resulting from expert validation was .93~1.00. For each item, ‘yes’ is 1 point and ‘no’ is 0 points, with a minimum of 0 points and a maximum of 8 points. A higher score indicated a higher degree of pregnancy-related anxiety in women with IBD. Kuder–Richardson 20 was .78 in this study.
4) General and disease-related characteristics
Referring to previous studies [22], general characteristics included age, marital status, education level, employment status, current plans for pregnancy, and the number of children wanted. The disease-related characteristics included IBD type, duration of IBD diagnosis, hospitalization experience, number of hospitalizations, operation experiences related to IBD, number of operations, and history of stoma.
5) Interview questionnaire
The first focus group interview (FGI) questions were “Why did you attend this program?”, “How do you feel about pregnancy?”, and “What do you feel after this week’s program?”. The questions in the second FGI were “Tell me how you managed your symptoms last week,” “What disease management behaviors have you changed since participating in the program last week?”, and “What does this program mean to you?”. For individual tele-coaching questions, the 5Rs coaching model developed by the Asia Coach Federation was used [23]. 5Rs coaching was employed to confirm participants’ IBD management ability after program, set behavioral change goals for the participant, and encourage health management behavior. The 5Rs of the model consist of 5 stages of questions to solve problems; 5Rs are the ‘relation’ stage to form relationships with participants, ‘refocus’ to find the goal, ‘reality’ to recognize the current situation, ‘resources’ stage, a process of participants finding answers on their own to solve a problem, and ‘responsibility’ stage where actions can be checked. Examples of questions used in this tele-coaching are provided in Supplementary Table 1. Women diagnosed with IBD and IBD experts reviewed the interview questions to determine whether the questions were appropriate for women with IBD.
4. Study intervention
1) The pre-conception care program for women with IBD
The PCCP-IBD was developed using Bandura’s [14] concepts of efficacy expectations, performance accomplishment, vicarious experience, verbal persuasion, and physiological states [24]. Strategies using self-efficacy resources in each content of the PCCP-IBD are well presented in Table 1. The content structure and number of sessions of this program were determined by expert opinions and pilot tests [24]. The program consisted of four sessions with the goal of maintaining remission before pregnancy. The educational content included information on IBD management, pre-conception management and contraception, management during pregnancy, delivery methods, breastfeeding, and IBD patients’ pregnancy experiences [24]. The methods used for the program were small group lectures, discussions, and video clips as well as individual tele-coaching. A pre-conception care diary was also provided to help participants manage their condition and prepare for pregnancy by recording their IBD symptoms, sleep times, moods, medications, and diet, as well as information about their menstrual cycles, sexual behaviors, and contraception (Supplementary Figure 1) [24]. The content validity of this PCCP-IBD and educational materials was verified by a group of experts. The expert group consisted of one nursing professor, one gastroenterology specialist, one IBD nurse specialist, two wound ostomy nurses, and two gastroenterology nurses with more than 10 years of experience. The CVI was calculated on a 4-point scale (1 = not appropriate, 4 = very appropriate) and according to the proportion of respondents who scored 3 or more points. The CVI for each item ranged from .79 to .96. Some minor revisions were made according to specific opinions from the experts. The program was modified based on the experts’ opinions, and a preliminary test was conducted on two women diagnosed with IBD. The material was finally completed after receiving feedback [24].
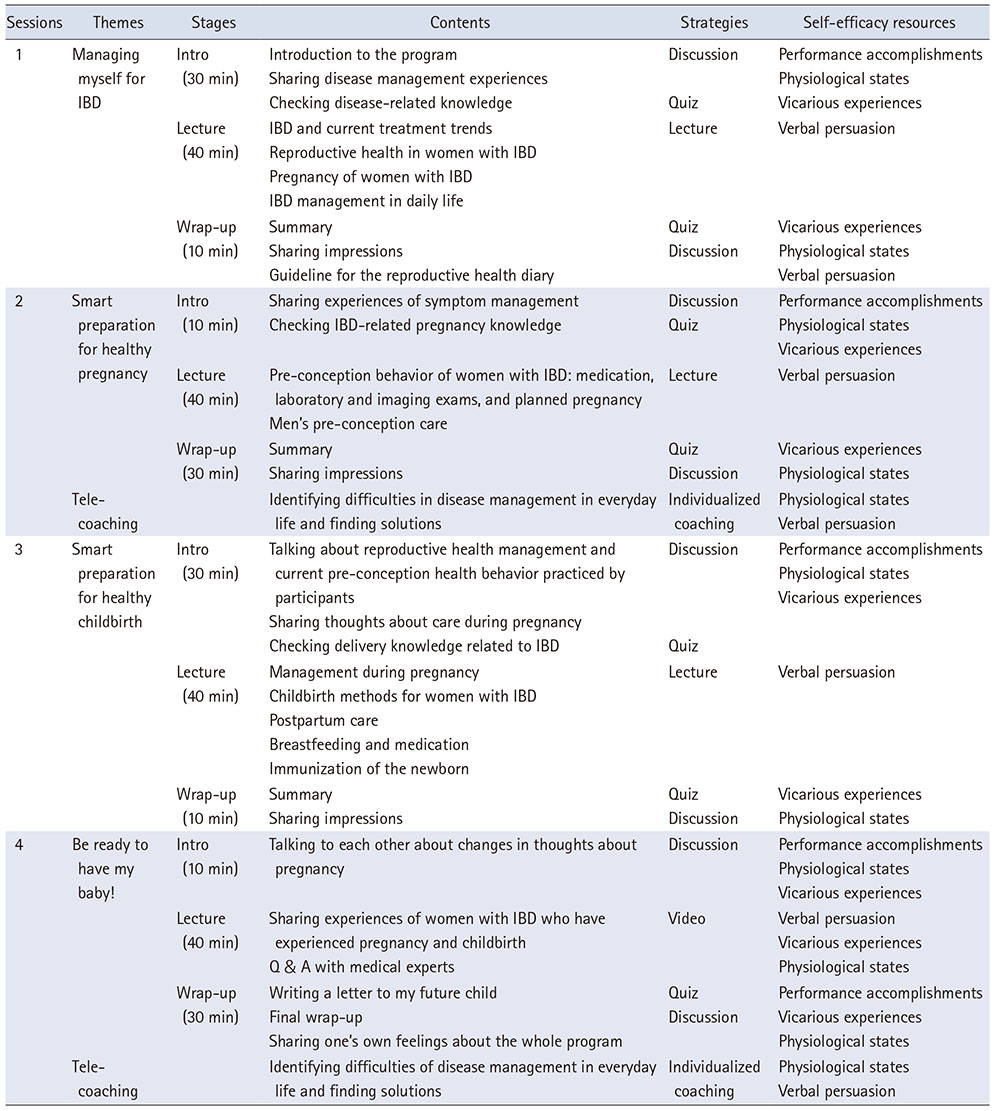
Table 1
The Content of the Pre-Conception Care Program for Women with IBD
Before operating the program, we collected opinions from patients with IBD who participated in a preliminary test and experts in IBD and education. Since most of the IBD patients were office workers or students, it was suggested to keep the program short. In addition, due to the outbreak of COVID-19, it was recommended to minimize the duration of the program. As a result, the program was set to two weeks, offering two sessions per day per week. Each session lasted for 80 minutes, and the small groups consisted of three to six participants. The small group education was conducted in the seminar room. Individual tele-coaching was conducted after every two sessions to check whether the participants understood the education content well, whether self-management was well performed, and whether their attitudes toward pregnancy had changed. During tele-coaching, additional education related to pregnancy was provided according to each individual’s situation. Encouragement and motivation were also provided to promote self-management by taking prescribed medications, exercising regularly, eating a healthy diet, and forth. It was a method that applied physiological states and verbal persuasion among self-efficacy enhancement strategies. A total of two tele-coaching sessions were conducted during the program, and the average time for each session was approximately 30 minutes (ranging from 20 to 40 minutes). Small group education and individual tele-coaching were conducted by the researcher.
2) IBD Management and Women’s Health
For the control group, ‘IBD Management and Women’s Health’ was provided in the form of small group education. Each group consisted of 3 to 7 participants, and it was provided twice, with each session lasting 60 minutes. The educational content covered various topics including IBD management, cervical cancer prevention, and menstrual disorders, which were already part of the hospital’s existing program. In this study, the control group was not on a waitlist, and the education was provided at the same time as the intervention group. Blinding of the participants was performed to control the maturation effect, which could be a threat to internal validity. After the all data collection was completed, the control group was provided with an educational booklet and the pre-conception care diary used in PCCP-IBD.
5. Data collection and procedure
Data collection for the intervention group and control group were conducted from February to April 2020. Quantitative data were collected at three different points: baseline (T0), one week after the program (T1), and four weeks after the program (T2). The initial data collection was conducted by a research assistant before the program started. After the program ended, the researcher collected data by sending a link to the online survey site via mobile text message. Participants who completed the online survey were restricted from duplicate responses. Participants took approximately 15 minutes to complete the questionnaire.
To qualitatively evaluate the effectiveness of the program, FGIs and individual tele-coaching were used to discuss the participants’ experiences before and after the program. All members of the intervention group participated in the FGI. The FGIs were conducted with a total of four intervention groups consisting of 6, 5, 3, and 3 participants, identical to the small group education. The researcher conducted four interviews per group (30 minutes each) at the beginning and end of the program. Permission to record the interviews was obtained from the participants in advance, and the interview process was audio-recorded and then analyzed. All participants in the intervention group also participated in individual tele-coaching.
6. Data analysis
1) Quantitative data analysis
The quantitative data were analyzed using IBM SPSS Statistics 25 (IBM Co.). General characteristics and disease-related characteristics were analyzed using descriptive statistics. Between-group homogeneity was analyzed using the chi-square test, Fisher’s exact test, independent t-test, and Mann–Whitney U-test. Between-group differences in outcome variables across time were analyzed using the generalized estimation equation (GEE) method. GEE is a method of applying multiple regression analysis in consideration of the intra-subject correlation of measured values. GEE can determine the interaction between time and group after controlling for the effect of the confounding variable. In addition, in GEE, the subject of analysis is not the individual but the observed value itself, so it is possible to analyze under the influence of missing values [25].
Variables with prior differences in homogeneity between the groups were analyzed as confounding variables. To confirm the effect size of the program on each outcome variable, partial eta squared (η2) was calculated using repeated measure ANOVA. Statistical significance for all tests was indicated by a two-tailed p-value <.050.
2) Qualitative data analysis
Qualitative data analysis was conducted using FGI transcripts and tele-coaching records through the deductive content analysis method [26].
After repeatedly reading the transcripts and coding them for meaningful words, phrases, and sentences related to the outcome variables of this study, sub-categories were abstracted and categorized.
To ensure the qualitative validity of the study results, the evaluation criteria of credibility, fittingness, auditability, and confirmability suggested by Sandelowski [27] were confirmed. To ensure credibility, at the end of each interview, the contents of the interview were summarized and validated by the participants. All interview data were recorded, listened to repeatedly, and transcribed promptly after the interview date to ensure the accuracy and completeness of the data, avoiding any distortion or omission. To ensure fittingness, we recruited women diagnosed with IBD who were registered at the hospital and had no childbirth experience and were randomly selected to reduce sampling bias. Data were collected until saturation was reached when no more information was available. The topics and specific narratives identified in the content analysis were confirmed through interviews with two participants. To improve the accuracy of the descriptions, a nurse at an IBD center identified topics that reflected the circumstances experienced by patients in clinical practice, and two nursing professors with experience in qualitative study conducted a review to see if the identified topics reflected the original data described. To ensure auditability, the qualitative study process, including a selection of participants, preparation of researchers, and construction of structured questionnaires, was described in detail. To ensure confirmability, we continuously checked for pre-conceptions or biases regarding participant statements and tried to maintain neutrality during the study process.
7. Ethical consideration
This study was approved by the Institutional Review Board of Asan Medical Center where participant recruitment took place, prior to data collection (document number: S2019-2572-0001). This study was registered on the Korea Clinical Trial Registration Site (Clinical Research Information Service) of the Centers for Disease Control and Prevention of the National Institute of Health (clinical trial registration number: KCT0008022; last verified in December, 2022). This clinical study did not involve invasive treatments or medications, so the risk that could arise from the study was low. However, since the study was conducted during the COVID-19 pandemic, there was a risk of infection through group education.
Therefore, we made every effort to prevent infection of the participants, such as measuring body temperature, hand washing, and wearing masks before and during the intervention. No damage or side effects occurred to the participants during the period of this study.
All participants were informed of the purpose, study procedures, benefits of the study, possible harms arising from the study, and that if they did not want to participate, they could withdraw at any time during the study process. The participants voluntarily signed the informed consent form. In addition, participants’ confidentiality and anonymity were protected, and collected data were stored in an encrypted file.
RESULTS
1. Quantitative finding
1) General and disease-related characteristics
A total of 35 women participated in this study. The average age was 30.3 years, and 42.9% were married. 57.1% were currently planned to become pregnant, and 54.3% wanted to have two or more children. Regarding disease-related characteristics, 62.9% were diagnosed with CD, and the average duration of IBD diagnosis was 9.2 years. 62.9% had been hospitalized, with an average of three hospitalizations. 40.0% of the participants had surgery due to disease, with an average of two surgeries and two women had an ostomy.
Significant differences between-group differences were found for current plans for pregnancy (p = .011) and the number of children wanted (p = .040). There were no significant differences in disease-related characteristics between the groups (Table 2).
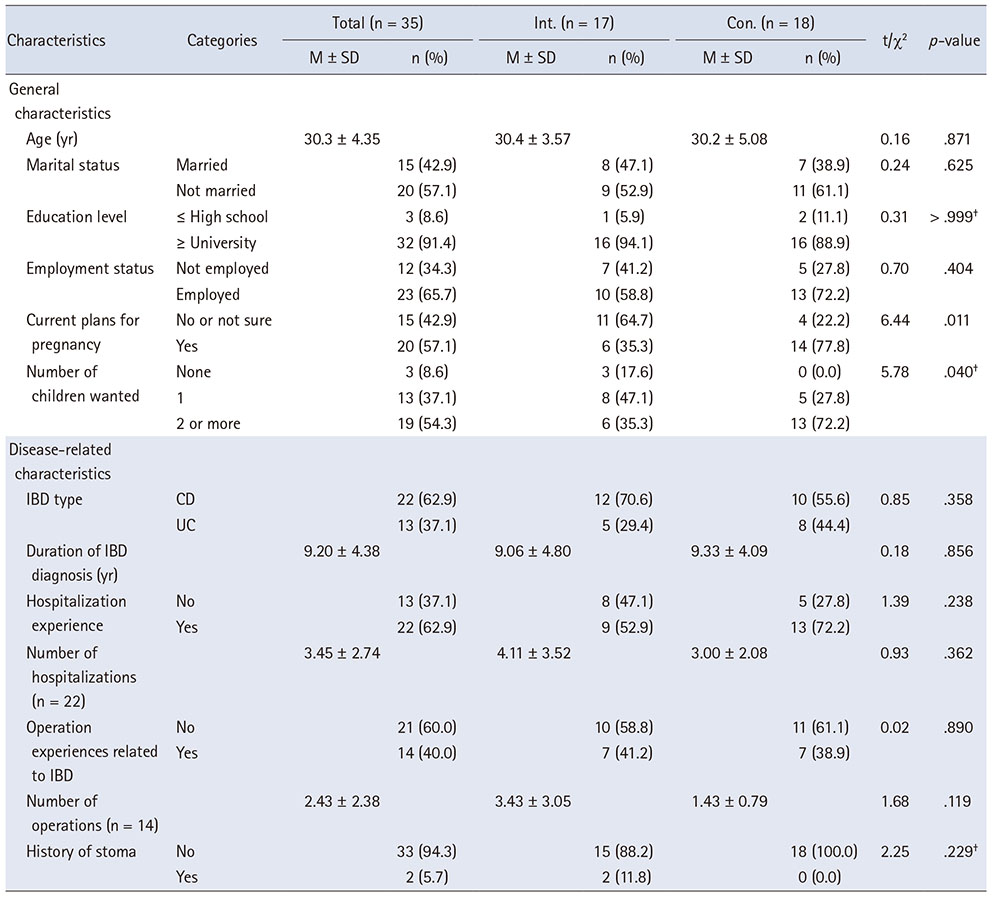
Table 2
Homogeneity Testing of General and Disease-Related Characteristics between the Intervention and Control Groups
2) Changes in self-efficacy for IBD management, IBD-related pregnancy knowledge, and IBD-related pregnancy anxiety
After completing the program, self-efficacy for IBD management showed a significant increase over time in the intervention group compared to the control group (Wald χ2 = 4.41, p = .036, partial η2 = .06). IBD-related pregnancy knowledge scores increased significantly over time in the intervention group (Wald χ2 = 13.80, p < .001, partial η2 = .22), and IBD-related pregnancy anxiety was found to significantly decrease over time in the intervention group (Wald χ2 = 8.61, p = .003, partial η2 = .12) (Table 3).
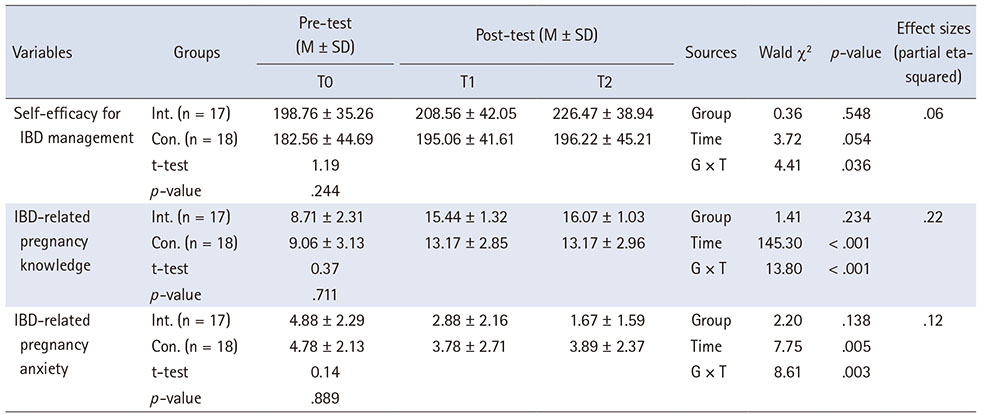
Table 3
Changes in Outcome Variables in the Two Groups after the PCCP-IBD
2. Qualitative finding
Three themes and seven sub-themes were identified. The themes were “improving confidence in IBD management and awareness for planned pregnancy,” “improving IBD awareness related to pregnancy and childbirth,” and “relieving anxiety about pregnancy and actively facing pregnancy.”
1) Improving confidence in IBD management and awareness of planned pregnancy
Participants recorded their IBD management behaviors in a diary and reflected on their shortcomings regarding IBD management. In addition, through the items written in the diary, the women began to learn and practice specific IBD management tools for pre-pregnancy remission and develop more confidence related to IBD management. They also began to take steps toward planned pregnancy by recording their reproductive health management practices.
(1) Gaining experience in symptom management
Participants were able to control their IBD symptoms while keeping a diary and felt a sense of accomplishment when looking at the completed diary every day. These positive experiences became a driving force for self-confidence.
I went to the outpatient clinic today, and the examination results have improved a lot. It’s the first time I’ve heard good news after an examination. It’s so good. I will continue to manage it well in the future. (Participant 6)
(2) Making efforts to maintain a healthy body
The women wanted to maintain their physical health. Participants who wished to become pregnant began to prepare for pregnancy by receiving pre-pregnancy vaccinations and reproductive system examinations. The PCCP-IBD provided an opportunity for participants to expand the scope of their healthcare needs.
I have had two bowel resections. So, I think I need to check the condition of my fallopian tubes for pregnancy. (Participant 8)
After this program, I finally got the cervical cancer vaccination, which I had been putting off until now. (Participant 10)
2) Improving IBD awareness related to pregnancy and childbirth
The second theme reflects participants’ increased awareness of IBD and its effects on pregnancy and childbirth. The participants said that the program was their first time receiving reproductive health education exclusively for women with IBD provided by experts and that the program provided specific and accurate information about pregnancy and childbirth with a focus on IBD.
(1) Resolving curiosity about pregnancy
The participants had questions about pregnancy and concerns about whether their reproductive health problems were related to IBD. Since the symptoms of IBD are very diverse, the participants faced difficulties meeting patients with similar symptoms and struggled with many of the same concerns. They were frustrated because they could not get clear answers from their gynecologists about IBD and pregnancy. Participation in the program resolved many of their doubts.
For the first time, I was able to acquire detailed and professional knowledge, from the most basic woman reproductive information to pre-pregnancy preparations, the pregnancy period and childbirth, and the final breastfeeding period. It was really necessary knowledge for women with IBD like me, and it really helped me to resolve my doubts. (Participant 6)
(2) Understanding IBD medication and pregnancy
Information on drugs for IBD that could be taken throughout pregnancy, postpartum, and during lactation including the latest drugs, was presented using easy-to-understand pictures, which participants found helpful.
There were things I knew and things I didn’t know, but there were a lot more things I didn’t know. The best thing about the section on medications was that I could understand their effects at a glance before, during, and after pregnancy. (Participant 13)
3) Relieving anxiety about pregnancy and actively facing pregnancy
After being diagnosed with IBD, participants felt vaguely anxious about pregnancy and often wished to avoid it. However, after participating in this program, they realized that they had misunderstood pregnancy, and they were able to relieve their worries about pregnancy and accepted pregnancy as a positive phenomenon.
(1) Shift in perspective of pregnancy
Before participating in the program, participants felt uncertainty about IBD and pregnancy, including fears of passing IBD on to their children and not being able to take IBD medication during pregnancy. Many participants chose to delay or avoid pregnancy due to the possible burden of raising children with chronic diseases. The program helped participants to realize that their passive and negative attitudes toward pregnancy were caused by unnecessary fear.
I think I was anxious and a little afraid during that time. Now, even with Crohn’s disease, I realize that I don’t have to worry so much. I feel a little more comfortable. (Participant 15)
(2) Expecting to become pregnant
Participants were assured that they could have a healthy pregnancy and childbirth, and their expectations about having children changed.
Well, after taking classes like this, I thought that I should have a (baby) in the near future. (Participant 11)
(3) Preparing for pregnancy brings new concerns
Another practical concern arose when the participants considered preparing for pregnancy. Participants who had given up on pregnancy due to repeated failed in vitro procedures and subsequently decided to try an in vitro procedure again after attending the program felt ambivalent about pregnancy.
I haven’t thought about pregnancy for a long time, but now I look back and see so many different processes… So… it’s a bit complicated. My thoughts about pregnancy keep changing. Emotions also change. (Participant 4)
DISCUSSION
As a result of this study, PCCP-IBD, using self-efficacy enhancement strategies, was effective in improving self-efficacy for IBD management. This supported the results of a previous study that showed that self-efficacy enhancement strategies had a positive effect on self-efficacy for IBD management [13]. It is meaningful that this program improved the participants’ confidence in disease management. The reason for these results is thought to be the effect of performance accomplishment, a strategy that allows participants to practice health behaviors on their own and directly experience change by filling out pre-conception care diary during the program. In addition, the vicarious experience, which indirectly allows participants to experience positive changes by sharing the experiences of other participants through small group discussions, and the physiological states, which provides encouragement through tele-coaching, are considered effective. In fact, the results of the interview content analysis showed that the participants experienced symptom relief through writing a diary and gained confidence and a sense of accomplishment in being able to manage it on their own. In particular, it was confirmed that the effect persisted even after four weeks of the program in the intervention group. This result shows that the self-efficacy for disease management that arises from experiencing symptom management can last for a long time. In the future, there is a need to conduct study to confirm whether the improvement in disease management self-efficacy through this program actually affects the disease-related behavior of women with IBD.
PCCP-IBD was effective in improving IBD-related pregnancy knowledge. In particular, one week after the end of the program, the knowledge score of the intervention group increased noticeably, which supports the results of previous studies that pregnancy-related education programs contributed to improving reproductive health knowledge in a short period of time [28, 29]. There was a significant difference in changes over time between the two groups. Education was provided through structured educational materials in each session, and the researcher’s answers to questions asked by participants during tele-coaching. It can be seen that the verbal persuasion strategy was effective. As a result of quantitative study, not only knowledge related to drugs, but also the relationship between disease inheritance and pregnancy, management during pregnancy, childbirth methods, and outcomes were improved. It was interpreted that awareness of the possibility of healthy pregnancy and childbirth among women with IBD has increased. Therefore, in the future, educational materials and education on pregnancy-related information desired by women with IBD should be actively provided.
This program effectively reduced IBD-related anxiety, and a significant decrease in anxiety was confirmed over time in the intervention group. In particular, anxiety levels remained low even after four weeks of the intervention. This reduction in anxiety is believed to be an effect of the vicarious experience strategy, which confirmed the successful pregnancy experience of patients in the last session through videos. This supports the previous research showing that self-efficacy-based educational intervention for pregnant women has a significant effect in reducing anxiety of pregnancy by providing vicarious experiences through a healthy role model [30]. During the interview, participants expressed that they had been unnecessarily worried due to incorrect knowledge through videos about the pregnancy experiences of women with IBD, including those with stomas, and that their thoughts about pregnancy had changed positively. However, unlike the quantitative research results showing that anxiety was continuously reduced, the qualitative research results confirmed that new practical concerns arose due to the participants’ difficult experience of infertility-related procedures. Accordingly, there is a need for increased attention to infertile women with IBD and the provision of patient-centered counseling and treatment, involving obstetricians and gastroenterologists.
However, when we further analyzed the changes in pregnancy-related anxiety of the participants by item, which was quantitative data, it was found that parenting-related anxiety persisted (Supplementary Table 2), potentially due to the perceived burden of raising children while managing IBD. It is known that women with disease experience more parenting stress than healthy women [31], and this stress can worsen IBD symptoms [32]. One study reported that disease activity increased within one year after giving birth in one-third of women with IBD [33]. Therefore, there is a need to consider developing programs for stress management in women with IBD during the postpartum period. In particular, disease activity during the postpartum period was found to increase in women whose disease was active before and during pregnancy [34]. This result confirms the importance of disease management before and during pregnancy. The program not only aims to maintain pre-pregnancy remission, but also includes information on disease management during pregnancy and the postpartum period. Therefore, it is believed that the PCCP-IBD program may also have an impact on the health of postpartum women.
Next, we discuss the application of the program conducted in this study. The age of the participants in this study was limited to adult women of childbearing age between 20 and 45 years. Participants were recruited regardless of whether they wished to become pregnant. Many women with IBD avoid pregnancy, and the purpose of pre-conception education is typically to prepare women physically and mentally for a healthy pregnancy, provide an opportunity for women to think about when to conceive, and avoid unwanted pregnancies [8]. Therefore, future studies should provide educational interventions tailored to participants’ intentions regarding pregnancy.
In this program, the small-group discussions provided an effective opportunity for indirect experiences. The participants in the groups were of a similar age, and all were concerned about pregnancy and women’s health, thus establishing a bond based on mutual concerns. These discussions may have prompted participants to reflect on their own healthcare and commence disease management. The facilitator flexibly reconfigured the goals and content of the sessions to suit the groups’ specific needs, thereby effectively providing customized education.
In particular, the advantage of this study is that individual tele-coaching was provided to gain an in-depth understanding of participants’ personal concerns that may not have been revealed in small group discussions. When participants who had experiences of infertility or failed procedures expressed complex feelings about pregnancy, the researcher accepted those feelings and encouraged those participants to thoroughly examine their emotions and make pregnancy decisions for themselves. These participants said that their fears were reduced after viewing their pregnancy from a neutral point of view. Individual coaching can provide opportunities to effectively address the complex psychological states of individual participants.
The pre-conception care diary provided to participants in this study helped participants to improve and maintain their health management behaviors by stimulating reflection. Participants expressed that the diaries were helpful for disease management and that they were willing to use them for future management. App-based diaries for IBD patients have recently been developed and used in other countries [35]. Therefore, patients utilizing the app-based diary for disease management may be useful for women with IBD preparing for pregnancy.
The main strength of this study is that, for the first time, a pre-conception care program tailored to the characteristics of the disease was developed and its effectiveness was confirmed for women of childbearing age diagnosed with a chronic disease. In particular, the advantage is that quantitative and qualitative methods were used to understand the women with IBD and confirm the effectiveness of the program. Qualitative data analysis confirmed that they started reproductive health care to prepare for their pregnancy, which was not highlighted in the quantitative study.
However, this study has some limitations. First, since the study participants were recruited at a single hospital, there are limitations in representing Korean women with IBD. Therefore, a repeat study targeting multicenter patients is needed in the future. Second, we did not examine whether the effectiveness of program differed depending on IBD type. Previous studies have shown that women with CD experienced more negative birth outcomes than women diagnosed with UC [3, 4]. This implies that women diagnosed with CD might have higher anxiety, but this study did not confirm that hypothesis. Therefore, future studies should attempt to determine whether the program effectiveness differs between women diagnosed with CD and those diagnosed with UC. Third, since this study also included women who did not necessarily intend to become pregnant, additional study is needed to clarify the effects of the intervention on women who are actually preparing for pregnancy or women who do not intend to become pregnant. Finally, the effectiveness of the program was assessed after one and four weeks. Therefore, in the future, long-term follow-up studies should be conducted to confirm how effective PCCP-IBD is in actual pre-conception management practices and for women with IBD during pregnancy and postpartum.
The number of women of childbearing age diagnosed with IBD is rapidly increasing in Korea. Nevertheless, there is a lack of education regarding pregnancy for women with IBD. Therefore, it is expected that the results of this study can be usefully applied to clinical practice, as follows: First, nurses can conduct education in the clinic using the educational booklet developed in this study when consulting young women with IBD about pregnancy. Second, the pre-conception care diary developed in this study can guide women with IBD to manage their own IBD and their reproductive health. Third, the content of this program will be developed as an online program, such as an application, in order to provide education without being limited by time and place. In addition, these materials can be used to educate medical staff who find it difficult to counsel IBD patients about reproductive health. Through various applications of this program, we believe that self-care can be enhanced by raising awareness about the importance of maintaining the remission period before pregnancy in women with IBD and by increasing self-efficacy in disease management. In addition, it is expected to reduce anxiety and shift their perspective of pregnancy and create a positive perception of pregnancy.
CONCLUSION
This study developed and applied a reproductive health education program for women of childbearing age diagnosed with IBD by applying Bandura’s [14] theory regarding resources for enhancing self-efficacy. Quantitative and qualitative data analyses confirmed that the program in this study was effective in enhancing self-efficacy for IBD management, IBD-related pregnancy knowledge, and reducing IBD-related pregnancy anxiety in women of childbearing age with IBD. This study makes a meaningful contribution from a practical point of view in that it developed and applied the first reproductive health education program for women of childbearing age with IBD in Korea. It is also essential that this educational program focusing on women’s health (specifically, IBD management before, during, and after pregnancy) and aiming to promote reproductive system health management was developed and provided by nurses. Furthermore, the booklets, pre-conception care diary, and educational materials used in this program can be utilized in a clinical setting. It is expected that reproductive health counseling and education by nurses will become more common in clinical practice in the future.
SUPPLEMENTARY DATA
Supplementary data to this article can be found online at https://doi.org/10.4040/jkan.24010.
Five Steps of Questions during the Individual Tele-CoachingSupplementary Table 1
Changes in IBD-related Pregnancy Anxiety after the PCCP-IBD in the Intervention GroupSupplementary Table 2
Parts of the educational material and pre-conception care diary.Supplementary Figure 1
Notes
CONFLICTS OF INTEREST:The authors declared no conflict of interest.
FUNDING:This study was supported by the National Research Foundation of Korea (NRF) grant funded by the Korean government (Grant No. 2018-R1A2B2-001231). This research was supported by the BK 21 Four Project (Center for World-Leading Human-Care Nurse Leaders for the Future) funded by the Ministry of Education (MOE, Korea) and National Research Foundation of Korea (NRF).
AUTHOR CONTRIBUTIONS:
Conceptualization or/and Methodology: Lee Y & Kim H.
Data curation or/and Analysis: Lee Y & Kim H & Kim Y & Yang S.
Funding acquisition: Kim H.
Investigation: Lee Y & Kim H & Kim Y & Yang S & Kim J.
Project administration or/and Supervision: Kim H.
Resources or/and Software: Lee Y & Kim Y & Yang S.
Validation: Lee Y & Kim H & Kim Y & Yang S & Kim J.
Visualization: Lee Y & Kim H & Kim Y & Yang S & Kim J.
Writing original draft or/and Review & Editing: Lee Y & Kim H & Kim Y & Yang S & Kim J.
ACKNOWLEDGEMENTS
None.
DATA SHARING STATEMENT
Please contact the corresponding author for data availability.
References
-
Park SH, Kim YJ, Rhee KH, Kim YH, Hong SN, Kim KH, et al. A 30-year trend analysis in the epidemiology of inflammatory bowel disease in the Songpa-Kangdong district of Seoul, Korea in 1986-2015. Journal of Crohn’s and Colitis 2019;13(11):1410–1417. [doi: 10.1093/ecco-jcc/jjz081]
-
-
O’Toole A, Nwanne O, Tomlinson T. Inflammatory bowel disease increases risk of adverse pregnancy outcomes: A meta-analysis. Digestive diseases and sciences 2015;60(9):2750–2761. [doi: 10.1007/s10620-015-3677-x]
-
-
Purewal S, Chapman S, Czuber-Dochan W, Selinger C, Steed H, Brookes MJ. Systematic review: The consequences of psychosocial effects of inflammatory bowel disease on patients’ reproductive health. Alimentary Pharmacology and Therapeutics 2018;48(11-12):1202–1212. [doi: 10.1002/ibd.20082]
-
-
Selinger CP, Eaden J, Selby W, Jones DB, Katelaris P, Chapman G, et al. Patients’ knowledge of pregnancy-related issues in inflammatory bowel disease and validation of a novel assessment tool (‘CCPKnow’). Alimentary Pharmacology Therapeutics 2012;36(1):57–63. [doi: 10.1111/j.1365-2036.2012.05130.x]
-
-
Yerushalmy-Feler A, Ron Y, Barnea E, Nachum A, Matalon S, Dali-Levy M, et al. Adolescent transition clinic in inflammatory bowel disease: Quantitative assessment of self-efficacy skills. European Journal of Gastroenterology and Hepatology 2017;29(7):831–837. [doi: 10.1097/meg.0000000000000864]
-
-
Bandura A. The explanatory and predictive scope of self-efficacy theory. Journal of Social and Clinical Psychology 1986;4(3):359–373. [doi: 10.1521/jscp.1986.4.3.359]
-
-
Magharei M, Jaafari S, Mansouri P, Safarpour A, Taghavi SA. Effects of self-management education on self-efficacy and quality of life in patients with ulcerative colitis: A randomized controlled clinical trial. International Journal of Community Based Nursing and Midwifery 2019;7(1):32–42. [doi: 10.30476/ijcbnm.2019.40844]
-
-
Creswell JW, Plano Clark VL, Gutmann ML, Hanson WE. Advanced mixed methods research designs. In: Tashakkori A, Teddlie C, editors. Handbook of Mixed Methods in Social and Behavioral Research. SAGE Publishing; 2003. pp. 209-240.
-
-
World Health Organization (WHO). Process of translation and adaptation of instruments [Internet]. WHO; c2018 [cited 2024 Mar 15].Available from: https://www.coursehero.com/file/30372721/WHO-
Process- of- translation- and- adaptation- of- instrumentspdf/.
-
-
Huang VWM. In: Reproductive knowledge specific to inflammatory bowel disease among women with IBD and physicians who treat women with IBD [master’s thesis]. Alberta (AB): University of Alberta; 2014. pp. 1-402.
-
-
Lee YJ, Oh EG. Body image, self esteem, and health related quality of life in patients with Crohn’s disease. Korean Journal of Adult Nursing 2014;26(4):383–392. [doi: 10.7475/kjan.2014.26.4.383]
-
-
Jeong P, Woo SM. In: 5R coaching leadership. Asia Coach Center; 2012. pp. 1-127.
-
-
Maeda E, Nakamura F, Kobayashi Y, Boivin J, Sugimori H, Murata K, et al. Effects of fertility education on knowledge, desires and anxiety among the reproductive-aged population: Findings from a randomized controlled trial. Human Reproduction 2016;31(9):2051–2060. [doi: 10.1093/humrep/dew133]
-
-
Mountifield R, Andrews JM, Bampton P. It IS worth the effort: Patient knowledge of reproductive aspects of inflammatory bowel disease improves dramatically after a single group education session. Journal of Crohn’s and Colitis 2014;8(8):796–801. [doi: 10.1016/j.crohns.2013.12.019]
-
-
Gandomi N, Sharifzadeh G, Torshizi M, Norozi E. The effect of educational intervention based on self-efficacy theory on pregnancy anxiety and childbirth outcomes among Iranian primiparous women. Journal of Education and Health Promotion 2022;11(1):14 [doi: 10.4103/jehp.jehp_1548_20]
-
-
Malhi G, Tandon P, Perlmutter JW, Nguyen G, Huang V. Risk factors for postpartum disease activity in women with inflammatory bowel disease: A systematic review and meta-analysis. Inflammatory Bowel Disease 2022;28(7):1090–1099. [doi: 10.1093/ibd/izab206]
-
 Cite
Cite
