 Submit an article
Submit an article
Search
- Page Path
- HOME > Search
Research Paper
- Development of a well-dying awareness scale for middle-aged adults in Korea: a mixed-methods study
- Yu Jin Jung, Eun Joung Choi
- J Korean Acad Nurs 2025;55(2):285-300. Published online March 28, 2025
- DOI: https://doi.org/10.4040/jkan.24121
-
 Abstract
Abstract
 PDF
PDF ePub
ePub - Purpose
This study aimed to develop a valid and reliable tool to measure awareness of well-dying among middle-aged adults.
Methods
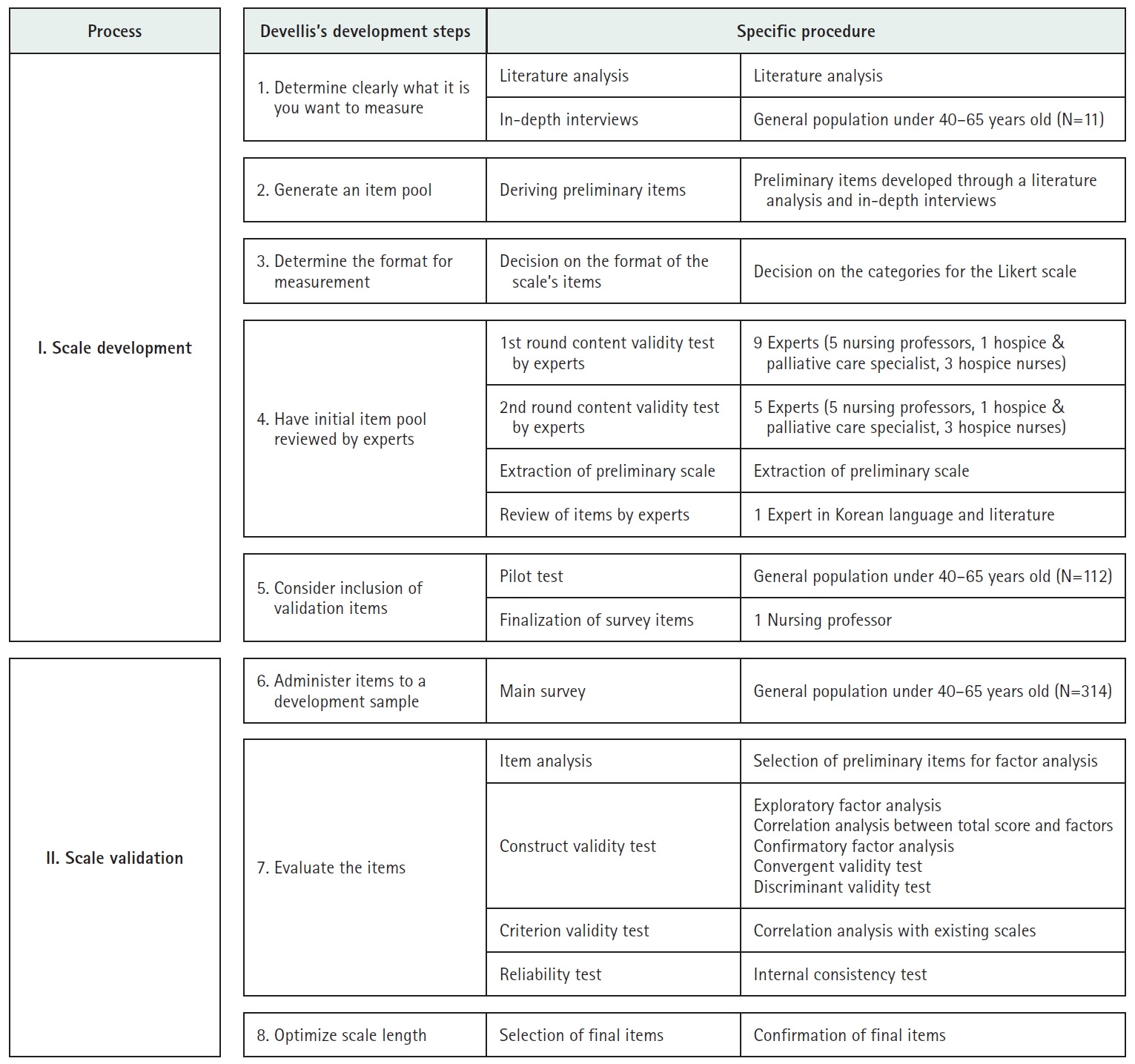
A mixed-methods approach was adopted, consisting of a qualitative phase to identify the characteristics of well-dying and a quantitative phase to validate the instrument with middle-aged participants. Initially, 76 items were generated through a literature review and in-depth interviews, and these were reduced to 35 items through expert validation. A pilot survey was conducted with 112 individuals aged 40–65, selected via quota sampling from 17 administrative regions in South Korea. Based on the pilot survey results, the instrument was refined to 32 items for the main survey. The main survey included 314 participants recruited through quota sampling in Busan and Ulsan Metropolitan Cities and Gyeongsang Region. Exploratory factor analysis (EFA), confirmatory factor analysis (CFA), and reliability testing were performed to validate the instrument.
Results
The final scale comprised 23 items across six factors. EFA demonstrated an explanatory power of 69.1%, with factor loadings ranging from 0.53 to 0.88. CFA confirmed the instrument’s validity, and reliability was established with a Cronbach’s α of .93.
Conclusion
This instrument is a validated and reliable tool for measuring middle-aged individuals’ awareness of well-dying. It can serve as an effective resource for evaluating and assessing well-dying awareness in the middle-aged population.
- 3,476 View
- 232 Download

Original Articles
- Effects of a Relapse Prevention Program on Insight, Empowerment and Treatment Adherence in Patients with Schizophrenia
- Jaewon Joung, Sungjae Kim
- J Korean Acad Nurs 2017;47(2):188-198. Published online April 28, 2017
- DOI: https://doi.org/10.4040/jkan.2017.47.2.188
-
Abstract
PDF
Purpose The purpose of this study was to develop a relapse prevention program (RPP) and examine the effects of the RPP on insight, empowerment, and treatment adherence in patients with schizophrenia.
Methods A non-equivalent control group pretest-posttest design was used. Participants were 54 inpatients who had a diagnosis of schizophrenia (experimental group: 26, control group: 28). The study was carried out from February 7, 2012 to February 6, 2013. Over a 10-day period prior to discharge each participant in the experimental group received three one-hour sessions of RPP a one-to-one patient-nurse interaction. Data were collected using Assess Unawareness of Mental Disorder (SUMD), Empowerment Scale, and Insight and Treatment Attitude Questionnaire (ITAQ) and analyzed using PASW 18.0 with chi-square test, independent t-test, Mann-Whitney U test, and ANCOVA.
Results The experimental group had a significant increase in insight and treatment adherence compared to the control group. However, there was no significant difference in empowerment between the two groups.
Conclusion Findings indicate that the RPP for patients with schizophrenia was effective in improving insight and treatment adherence. A longitudinal study is needed to confirm the persistence of these effects of RPP in patients with schizophrenia.
-
Citations
Citations to this article as recorded by
- Narrative Inquiry into Young Adults with Schizophrenia: A Journey of Variations in Hope
Jaewon Joung, Sungjae Kim
Journal of Korean Association for Qualitative Research.2025; 10(3): 179. CrossRef - Effects of a nonviolent communication-based anger management program on psychiatric inpatients
Jiyeon Kim, Sungjae Kim
Archives of Psychiatric Nursing.2022; 41: 87. CrossRef - Effects of Adherence to Pharmacological Treatment on the Recovery of Patients with Schizophrenia
Alejandra Caqueo-Urízar, Alfonso Urzúa, Patricio Mena-Chamorro, Josefa Bravo de la Fuente
Healthcare.2021; 9(9): 1230. CrossRef - Development and Effects of an Acceptance Commitment-based Cognitive Behavioral Program for Patients with Schizophrenia
Jae Woon Lee, Hyun Sook Park
Journal of Korean Academy of Psychiatric and Mental Health Nursing.2018; 27(4): 342. CrossRef - Effects of an Empowerment Program for Patients with Schizophrenia
Ju Hyun Woo, Ji Hye Jang, Jeong Hee Cho
Journal of Korean Academy of Psychiatric and Mental Health Nursing.2018; 27(2): 123. CrossRef - The Effects of Group Motivational Interviewing Compliance Therapy on Drug Attitude, Medicine Application Self-efficacy and Medicine Application in Psychiatric Patients
Dawoon Lee, Sungjae Kim
Journal of Korean Academy of Psychiatric and Mental Health Nursing.2017; 26(4): 391. CrossRef
- Narrative Inquiry into Young Adults with Schizophrenia: A Journey of Variations in Hope
- 1,625 View
- 25 Download
- 6 Crossref
- The Effect of Behavior Modification on Enhancing Patient Adherence to Tuberculosis Treatment Regimens
- Eun Lee Chung
- Journal of Nurses Academic Society 1996;26(3):697-708. Published online March 30, 2017
- DOI: https://doi.org/10.4040/jnas.1996.26.3.697
-
Abstract
PDF
Most efforts to improve tuberculosis treatment adherence target the patient and his or her behavior. This study examined the effects of behavioral modification training for these patients. Based on Bandura's behavioral principles of modeling, intervention strategies using a video program were devised to elicit specific patient target behaviors considered to improve patients' adher ence to tuberculosis treatment regimens. A random assignment, two-group (experimental group and control group) research design including 81 subjects was used. The main outcomes measured were pill taking measured with the Medication Event Monitaring System(MEMS) Medication Cap, patients' self-efficacy, and their knowledge of tuberculosis. The findings are as follows: 1) There was a significant difference between the experimental group and the control group in patients' feelings of self-efficacy. That is, the patients who received the behavior modification program showed greater feeling of self-efficacy to initiate and change their behavior for the tuberculosis treatment regimen than the patients who did not receive the program(t=3.51, p=0. 01). 2) There was a significant difference between the experimental group and the control group in patients' knowledge of tuberculosis. That is, the patients who received the behavior modification program showed higher level of knowledge of tuberculosis than the patients who did not receive the program(t=2.15, p=0.03). 3) There was a significant difference between the experimental group and the control group in patients' adherence to tuberculosis treatment regimens. That is, the patients who received the behavior modification program showed greater adherence to the treatment regimens than the patients who did not receive the program(t=5.11, P=0.00). The study findings provided useful insights into nursing practice, particularly in planning intervention strategies aimed at enhancing patients' adherence in tuberculosis that may also be relevant to other chronic diseases with patient adherence problems.
-
Citations
Citations to this article as recorded by- A Study on Multicultural Mothers’ Comprehension and Satisfaction with Language Screening Test Applications by Type of Information Provision
Eun Jin Lee, Ji-Hye Jeon, Ki-Hyung Hong, Young Tae Kim
Communication Sciences & Disorders.2023; 28(2): 386. CrossRef
- A Study on Multicultural Mothers’ Comprehension and Satisfaction with Language Screening Test Applications by Type of Information Provision
- 837 View
- 2 Download
- 1 Crossref
- A Survey on the Delay Time Before Seeking Treatment and Clinical Symptoms in Patients with Acute Myocardial Infarction
- Oh Jang Park, Cho Ja Kim, Hyang Yeon Lee, Hae Ok Lee
- Journal of Korean Academy of Nursing 2000;30(3):659-669. Published online March 29, 2017
- DOI: https://doi.org/10.4040/jkan.2000.30.3.659
-
Abstract
PDF
Many patients of acute myocardial infarction showed delay time before seeking treatment although they needed immediate thrombolytic therapy once they perceived their symptoms. The objectives of this study were to identify the relationship between clinical symptoms and the delay, and to find the time spent before seeking the treatment. This study was a retrospective research. The delay time for the treatment consisted of the length of delay from symptom onset to patients' decision (T1), from patients' decision making to finding transportation (T2), and from taking transportation to the first hospital arrival(T3). The subjects were 89 patients who were admitted in the ICU and Cardiac Ward at Chonnam University Hospital with the first attack of acute myocardial infarction. The data was collected for three months from March 1st to May 31st of 1998 through questionnaires and reviewing patients' charts: The chart information was suppled by two nurses working at the ICU and Cardiac Ward. The data was analyzed by using frequency, mean and ANOVA through the SAS program. The results of study summarized as follows: 1. Sixty two patients (69.7%) were male and twenty seven patients (30.3%) were female, the ratio of male to female was 2.3 : 1. 2. In daily life, the 70.8% of the patients felt chest pain and discomfort fatigue in 67.4%, dyspnea in 57.3%, and pain in arm, neck, and jaw in 52.8%. During the attack, 97.8% of the patients felt chest pain and discomfort dyspnea in 82.1%, pain in arm, neck, jaw in 67.4% and perspiration in 51.7%. 3. The length of time a patient spent seeking time for treatment (T1+T2+T3) was 94.6 minutes, in which the time for patients' decision making for treatment (T1) was 70.3 minutes, time for finding transportation (T2) was 8.2 minutes, and time for the transportation of the patient to the first hospital (T3) was 16.1 minutes. Time for patients' decision making to go to a hospital(T1) was 74.2% of the total time sought for treatment.
-
Citations
Citations to this article as recorded by- Decision Tree Model of the Treatment-Seeking Behaviors Among Korean Cancer Patients
Hyo-Sook Oh, Hyeoun-Ae Park
Cancer Nursing.2004; 27(4): 259. CrossRef
- Decision Tree Model of the Treatment-Seeking Behaviors Among Korean Cancer Patients
- 941 View
- 2 Download
- 1 Crossref
- Treatment-seeking Behavior among those with Signs and Symptoms of Acute Myocardial Infarction
- Cho Ja Kim, Gi Yon Kim
- Journal of Korean Academy of Nursing 1999;29(3):605-613. Published online March 29, 2017
- DOI: https://doi.org/10.4040/jkan.1999.29.3.605
-
Abstract
PDF
The main purposes of this study were to determine the interval between the onset of symptoms of myocardial infarction and treatment-seeking time and identify the factors related to the interval time. This study used a retrospective design, The sample consisted of 45 patients aged over 30 who were diagnosed with an acute myocardial infarction at two large university affiliated medical center from September 1, 1997 to June 30, 1998. Data was collected by using questionnaires, which included demographic data, premonitory clinical signs and symptoms of myocardial infarction, and a measure of the severity of the signs and symptoms. Also semi-structured interviews and chart reviews were used to obtain information related to treatment seeking time. The results of this study are summarized as follows: 1. The most frequent premonitory clinical symptom was chest pain(92.9%), the second, was perspiration(81.0%), and the next were nausea(40.5%) and dyspnea(38.1%). Thirty two patients reported having more than four premonitory signs and symptoms. Patients described the characteristics of chest pain as "something very heavy pressing down "(26.2%), "felt like my chest would burst"(24.4%), or "sharp pain"(16.7%). Over 95% of the sample reported having chest pain. 2. Twenty two (52.4%) patients reported to have "very severe" premonitory pain. 3. The mean time interval between the onset of signs and symptoms and the arrival at the medical center was 6.39+/-0.80 hours in 42 samples, the mean time from the onset to arrival at a local hospital was 3.27+/-.39 hours and for transfer from a local hospital to the medical center was 4.75+/-.87 hours in patients who had arrived at medical center via local hospital. 4. The severity of premonitory signs and symptoms did not differ significantly according to existence of premonitory signs and symptoms. 5. There was no significant relationship between treatment-seeking time and age, gender, marital status, economic status, occupation, or residence. But education had significant relationship(r=-0.51, p=0.01). Analysis of difference of the time interval according to the premonitory signs and symptoms showed that the time was shorter in patients who experienced nausea or dysnea(U=115.50, p=0.01, U=132.00, p=0.04), however the severity of premonitory signs and symptoms did not have statistical significance.
-
Citations
Citations to this article as recorded by- Factors associated with needlestick and sharp injuries among hospital nurses: A cross-sectional questionnaire survey
Eunhee Cho, Hyeonkyeong Lee, Miyoung Choi, Su Ho Park, Il Young Yoo, Linda H. Aiken
International Journal of Nursing Studies.2013; 50(8): 1025. CrossRef - Morbidity and mortality rates in women with heart disease: Lessons in gender differences from Korea
Myoung-Ae Choe, Kyungeh An
Contemporary Nurse.2003; 14(2): 158. CrossRef
- Factors associated with needlestick and sharp injuries among hospital nurses: A cross-sectional questionnaire survey
- 991 View
- 3 Download
- 2 Crossref
- The Comparison of the Effectiveness of Pelvic Floor Muscle Exercise and Biofeedback Treatment for Stress Incontinence in Korean Women
- Young Hee Choi, Myung Sook Sung, Jae Yup Hong
- Journal of Korean Academy of Nursing 1999;29(1):34-47. Published online March 29, 2017
- DOI: https://doi.org/10.4040/jkan.1999.29.1.34
-
Abstract
PDF
This study evaluated the Comparison of the Effectiveness of Pelvic Floor Muscle exercise and Biofeedback treatment for Genuine Stress Incontinence I assigned 60 participants to 2 groups : 30 to the pelvic floor muscle exercise group and 30 to the biofeedback group. Treatment protocol lasted for 6 weeks. Peak pressure, and duration time of pelvic muscle contraction were evaluated by a perineometer. Lower urinary symptoms, sexual matter and life style scores were achieved by using Jackson's scale. The treatment efficacy of the pelvic floor muscle exercise is compared with the biofeedback group and the main results of the comparison are as follows: 1. Pelvic muscle contraction 1) The peak pressure in the biofeedback group was significantly increased(P=0.000). 2. The frequency and quantity of incontinence 1) The frequency of incontinence in the biofeedback group was significantly decreased(P=0.000). 2) The quantity of incontinence in the biofeedback group was significantly decreased(P=0.000). 3. The lower urinary symptoms Daily frequency(P=0.000), nocturia(P=0.000), urgency(P=0.000), bladder pain(P=0.000), unexplained incontinence(P=0.048), wearing protection(P=0.022), changing outer clothing(P=0.005), hesitancy(P=0.008), intermittent stream(P=0.000), abnormal strength of stream(P=0.004), retention(P=0.000), incomplete emptying(P=0.000), and inability to stop mid steam(P=0.006) of the lower urinary symptoms in the biofeedback group were significantly decreased. 4. The sexual matters The dry vagina(P=0.004) and pain during sexual intercourse(P=0.002) in the biofeedback group was significantly decreased. 5. The life style. The fluid intake restriction(P=0.007), affected daily task(P=0.003), avoidance of places & situation(P=0.003), interference in Physical activity(P=0.002), interference in relationship with other people(P=0.01), and feeling about the rest of life with urinary symptom(P=0.000) in the biofeedback group were significantly decreased. In conclusion, the biofeedback treatment was more effective than the pelvic floor muscle exercise in genuine stress incontinence.
-
Citations
Citations to this article as recorded by- Effect of Pila-dance to Ease Urinary Incontinence of Middle-aged Women
Hye-Jeon Hong
The Korean Journal of Physical Education.2018; 57(2): 431. CrossRef - The Convergence Study on the Effects of Three Pelvic Floor Muscle Excercise on Thickness of Pelvic Floor Muscle and Abdominal Muscles
Si-Eun Kang, Jae-Hoon Shim, Sung-Dae Choung
Journal of the Korea Convergence Society.2016; 7(1): 105. CrossRef - Effect of Moxibustion at Junggeuk(CV3), Singwol(CV8) on Women's Urinary Incontinence and Quality of Life
Eun-Sook Lee, Yi-Soon Kim, Jeong-Won Lee, Mi-Jung Oh, Gyeong-Cheol Kim
Korean Journal of Acupuncture.2013; 30(3): 193. CrossRef - Effects of an Incontinence Prevention Program on Postpartum Women
Nam Ok Jeong
Korean Journal of Women Health Nursing.2009; 15(3): 177. CrossRef
- Effect of Pila-dance to Ease Urinary Incontinence of Middle-aged Women
- 1,030 View
- 1 Download
- 4 Crossref
- Effect of Endurance Exercise during Dexamethasone Treatment on the Attenuation of Atrophied Hind-limb Muscle Induced by dexamethasone in Rats
- Myoung Ae Choe
- Journal of Korean Academy of Nursing 1998;28(4):893-907. Published online March 29, 2017
- DOI: https://doi.org/10.4040/jkan.1998.28.4.893
-
Abstract
PDF
The purpose of this study was to determine the effect of regular exercise during dexamethasone injection in the body weight, weight of hind-limb muscles, myofibrillar protein content and glutamine synthetase activity. 180-200g female Wistar were divided into four groups: control, exercise, dexamethasone injection(dexa), and exercise during dexamethasone injection(D+E) group. The dexa group received daily subcutaneous injection of dexamethasone at a dose of 4mg/kg body weight for 7days. The exercise group ran on a treadmill for 60min/day(20minutes every 4 hours) at 10m/min and a 10degrees grade. The control group received daily subcutaneous injection of normal saline at a dose of 4mg/kg body weight for 7 days. The D+E group ran on a treadmill for 60min/day(20minutes every 4 hours) at 10m/min and a 10degrees grade during dexamethasone injection. Body weight of the control group increased significantly from days of experiment, that of the dexa group decreased significantly from day 4 of the dexa group decrease significantly from day 4 of the experiment resulting in a 82.4% decrease compared to the first day of the experiment. Body weight of the D+E group decrease significantly from day 5 of experiment resulting in a 81.77% decrease compared to the first day of the experiment. Body weights, muscle weight and myofibrillar protein content of the plantaris and gastrocnemius decrease significantly and muscle weight of the sleys tended to decrease with dexamethasone injection. Glutamine synthetase activity of the hind-limb muscles increase significantly with the dexamethasone injection. The relative weight of the soleus was comparable to the control group and that of plantaris decrease significantly and that of gastrocnemius tended to decrease compared to that of the control in the dexa group. Body weight and muscle weight of the plantaris and gastronemius of the exercise group were comparable to the control group, and the muscle weight of soleus showed a tendency to increase. The relative weight of the soleus increased significantly and that of the plantaris and gastrocnemius were comparable to the control in the exercise group. Myofibrillar protein content of the soleus and plantaris increased significantly and there was no change of GS activity of the hind-limb muscles compared to the control in the exercise group. Body weight of the D+E group was comparable to the dexa group, muscle weight of the hind-limb muscles increased significantly. Myofibrillar protein content of the soleus and plantaris increase significantly and that of the gastrocnemius tendency to increase compared to the dexa group. Body weight and muscle weight of the plantaris and gastrocnemius of the D+E group did not recover to that of the control group. Muscle weight of the soleus recovered to that of the control group. The relative weight and myofibrillar protein content of the hind-limb muscles recovered to that of the control group. From these results, it is suggested that regular exercise during dexamethasone injection might attenuate the muscle atrophy of the hind-limb muscles.
-
Citations
Citations to this article as recorded by- Effect of DHEA Administration Alone or Exercise combined with DHEA before Steroid Treatment on Rat Hindlimb Muscles
Myoung-Ae Choe, Gyeong-Ju An
Journal of Korean Academy of Nursing.2009; 39(3): 321. CrossRef
- Effect of DHEA Administration Alone or Exercise combined with DHEA before Steroid Treatment on Rat Hindlimb Muscles
- 1,184 View
- 9 Download
- 1 Crossref
- Pre- and In-Hospital Delay in Treatment and in-Hospital Mortality after Acute Myocardial Infarction
- Kyuneh An, Bongyeun Koh
- Journal of Korean Academy of Nursing 2003;33(8):1153-1160. Published online March 28, 2017
- DOI: https://doi.org/10.4040/jkan.2003.33.8.1153
-
Abstract
PDF
Purpose 1) To identify the time taken from symptom onset to the arrival at the hospital (pre-hospital delay time) and time taken from the arrival at the hospital to the initiation of the major treatment (in-hospital delay time) 2) to examine whether rapid treatment results in lower mortality. 3) to examine whether the pre- and in-hospital delay time can independently predict in-hospital mortality.
Methods A retrospective study with 586 consecutive AMI patients was conducted.
Results Pre-hospital delay time was 5.25 (SD=10.36), and in-hospital delay time was 1.10 (SD=1.00) hours for the thrombolytic therapy and 50.24 (SD=121.18) hours for the percutaneous transluminal coronary angioplasty(PTCA). In-hospital mortality was the highest when the patients were treated between 4 to 48 hours after symptom onset using PTCA (rho=.02), and when treated between 30 minutes and one hour after hospital arrival using thrombolytics (rho=.01). Using a hierarchical logistic regression model, the pre- and in-hospital delay times did not predict the in-hospital mortality.
Conclusion Pre- and in-hospital delay times need to be decreased to meet the desirable therapeutic time window. Thrombolytics should be given within 30 minutes after arrival at the hospital, and PTCA should be initiated within 4 hours after symptom onset to minimize in-hospital mortality of AMI patients.
-
Citations
Citations to this article as recorded by- Comparison of Clinical Manifestations and Treatment-Seeking Behavior in Younger and Older Patients with First-time Acute Coronary Syndrome
Seon Young Hwang
Journal of Korean Academy of Nursing.2009; 39(6): 888. CrossRef
- Comparison of Clinical Manifestations and Treatment-Seeking Behavior in Younger and Older Patients with First-time Acute Coronary Syndrome
- 816 View
- 3 Download
- 1 Crossref
- The Effect of Dialysate Flow Rate on Dialysis Adequacy and Fatigue in Hemodialysis Patients
- Sun Mi Cha, Hye Sook Min
- J Korean Acad Nurs 2016;46(5):642-652. Published online October 31, 2016
- DOI: https://doi.org/10.4040/jkan.2016.46.5.642
-
Abstract
PDF
Purpose In this single repeated measures study, an examination was done on the effects of dialysate flow rate on dialysis adequacy and fatigue in patients receiving hemodialysis.
Methods This study was a prospective single center study in which repeated measures analysis of variance were used to compare Kt/V urea (Kt/V) and urea reduction ratio (URR) as dialysis adequacy measures and level of fatigue at different dialysate flow rates: twice as fast as the participant’s own blood flow, 500 mL/min, and 700 mL/min. Thirty-seven hemodialysis patients received all three dialysate flow rates using counterbalancing.
Results The Kt/V (M±SD) was 1.40±0.25 at twice the blood flow rate, 1.41±0.23 at 500 mL/min, and 1.46±0.24 at 700 mL/min. The URR (M±SD) was 68.20±5.90 at twice the blood flow rate, 68.67±5.22 at 500 mL/min, and 70.11±5.13 at 700 mL/min. When dialysate flow rate was increased from twice the blood flow rate to 700 mL/min and from 500 mL/min to 700 mL/min, Kt/V and URR showed relative gains. There was no difference in fatigue according to dialysate flow rate.
Conclusion Increasing the dialysate flow rate to 700 mL/min is associated with a significant nicrease in dialysis adequacy. Hemodialysis with a dialysate flow rate of 700 mL/min should be considered in selected patients not achieving adequacy despite extended treatment times and optimized blood flow rate.
-
Citations
Citations to this article as recorded by- The Effect of Uncertainty on the Physiological Indexes of Hemodialysis Patients: Serial Mediating Effects of Uncertainty Appraisal and Self-care Behavior
Mi Kyung Kim, Eun Hee Jang
Korean Journal of Adult Nursing.2022; 34(1): 51. CrossRef - Fuzzy-based modeling and speed optimization of a centrifugal blood pump using a modified and constrained Bees algorithm
Omer Incebay, Ahmet Onder, Muhammed Arif Sen, Rafet Yapici, Mete Kalyoncu
Computer Methods and Programs in Biomedicine.2022; 221: 106867. CrossRef - Relationship of Symptom Clusters, Compliance with the Patient’s Role Behavior, and Dialysis Adequacy with Quality of Life in Hemodialysis Patients
Semi Moon, Chiyoung Cha
Journal of Korean Academy of Fundamentals of Nursing.2022; 29(3): 295. CrossRef - Pharmacokinetic and Pharmacodynamic Analysis of Critically Ill Patients Undergoing Continuous Renal Replacement Therapy With Imipenem
Zhe Li, Jing Bai, Aiping Wen, Su Shen, Meili Duan, Xingang Li
Clinical Therapeutics.2020; 42(8): 1564. CrossRef - FINITE ELEMENT ANALYSIS FOR COMPARING THE PERFORMANCE OF STRAIGHT AND UNDULATED FIBERS IN ALTERING THE FILTERING EFFICIENCY OF HEMODIALYZER MEMBRANES
M. S. SANGEETHA, A. KANDASWAMY, C. LAKSHMI DEEPIKA, C. V. REVANTH
Journal of Mechanics in Medicine and Biology.2019; 19(05): 1850063. CrossRef - Factors Influencing Sick Role Behavior Compliance in Patients on Hemodialysis
Hyun Mi Jeon, Hye Sook You
Journal of Korean Academy of Fundamentals of Nursing.2019; 26(1): 23. CrossRef
- The Effect of Uncertainty on the Physiological Indexes of Hemodialysis Patients: Serial Mediating Effects of Uncertainty Appraisal and Self-care Behavior
- 2,381 View
- 26 Download
- 6 Crossref
- Gender Difference in Osteoporosis Prevalence, Awareness and Treatment: Based on the Korea National Health and Nutrition Examination Survey 2008~2011
- Yunmi Kim, Jung Hwan Kim, Dong Sook Cho
- J Korean Acad Nurs 2015;45(2):293-305. Published online April 30, 2015
- DOI: https://doi.org/10.4040/jkan.2015.45.2.293
-
Abstract
PDF
Purpose The aim of the study was to assess and identify gender differences in factors associated with prevalence, awareness, and treatment of osteoporosis.
Methods Data for 3,071 men and 3,635 women (age≥ 50) from the Korea National Health and Nutrition Examination Survey 2008~2011 were included. Osteoporosis was defined by World Health Organization T-score criteria. Impact factors and odds ratios were analysed by gender using multivariate logistic regression.
Results Osteoporosis prevalence rates were 7.0% in men and 40.1% in women. Osteopenia rates were 45.5% and 46.0% respectively. Among respondents with osteoporosis, 7.6% men and 37.8% women were aware of their diagnosis. Also 5.7% men with osteoporosis and 22.8% women were treated. Higher prevalence was found among respondents who were older, at lower socioeconomic levels, with lower body mass index and shorter height in both genders, and among women with fracture history, and non-hormonal replacement therapy. Awareness and treatment rates for the risk groups were similar compared to the low risk controls for both genders. Fracture history increased awareness and treatment rates independently for both genders. Women with perceived poor health status and health screening had increased awareness and treatment rates, but not men.
Conclusion Results indicate that postmenopausal women have a higher prevalence of osteoporosis than men and awareness and treatment rates were higher than for men. Despite gender difference in prevalence, osteoporosis was underdiagnosed and undertreated for both genders. Specialized public education and routine health screenings according to gender could be effective strategies to increase osteoporosis awareness and treatment.
-
Citations
Citations to this article as recorded by- Evaluation of radiation dose to Korean population by general radiography
Hyung Woo Nam, Min Woo Kwak, Shin Dong Lee, Ju Young Kim, Kwang Pyo Kim
Nuclear Engineering and Technology.2025; 57(4): 103286. CrossRef - Effects of Gender-Specific Differences on Anthropometric Measurements and Blood Lipid Levels in Fatty Liver Grades
Youl-Hun Seoung
Journal of Radiological Science and Technology.2025; 48(1): 55. CrossRef - Exposure and health effects follow-up study of residents near a former smelter site
Young-Hun Kim, Da-Som Lee, Jung-Eum Lee, Heon Kim, Yong-Dae Kim, Young-Seoub Hong, Jung-Duck Park, Byung-Sun Choi
Toxicological Research.2025; 41(5): 523. CrossRef - A Study of Prevalence and Awareness of Low Bone Density of Female Utilizing Dental Panoramic Radiographs
Sung Jin Kim, In-Ja Song, Eun Joo Lee, Suk-Ja Yoon
The Korean Journal of Oral and Maxillofacial Pathology.2024; 48(3): 23. CrossRef - A Study of the Relationship Between Kidneys, Bones, and Teeth in Eastern-Western Medicine
Eun Bi Lee, Sang Yun Han
Journal of Physiology & Pathology in Korean Medicine.2024; 38(5): 187. CrossRef - Association between dietary intake of α-tocopherol and cadmium related osteoporosis in population ≥ 50 years
Renjia Li, Hai Qu, Jinwei Xu, Huiqin Yang, Jinyao Chen, Lishi Zhang, Jiuming Yan
Journal of Bone and Mineral Metabolism.2023; 41(4): 501. CrossRef - Tenofovir disoproxil fumarate versus tenofovir alafenamide on risk of osteoporotic fracture in patients with chronic hepatitis B: A nationwide claims study in South Korea
Eunju Kim, Hyun Woong Lee, Soon Sun Kim, Eileen Yoon, Eun Sun Jang, Jong‐In Chang, Young Youn Cho, Gi Hyeon Seo, Hyung Joon Kim
Alimentary Pharmacology & Therapeutics.2023; 58(11-12): 1185. CrossRef - Effect of
Spatholobus Suberectus Extract (SSE) on RANKL-treated RAW264.7 and LPS-induced Bone Loss
Dae Joong Lee, Jong Hyun Hwang, Do Hwi Park, Ki Sung Kang, Chan Yong Jeon, Gwi Seo Hwang
The Journal of Internal Korean Medicine.2022; 43(6): 1134. CrossRef - Efficient estimators with categorical ranked set samples: estimation procedures for osteoporosis
Armin Hatefi, Amirhossein Alvandi
Journal of Applied Statistics.2022; 49(4): 803. CrossRef - Up-to-Date Knowledge on Osteoporosis Treatment Selection in Postmenopausal Women
Hye Gyeong Jeong, Min Kyung Kim, Hee Jeung Lim, Seul Ki Kim
Journal of Menopausal Medicine.2022; 28(3): 85. CrossRef - Association of Dietary Total Antioxidant Capacity with Bone Mass and Osteoporosis Risk in Korean Women: Analysis of the Korea National Health and Nutrition Examination Survey 2008–2011
Donghyun Kim, Anna Han, Yongsoon Park
Nutrients.2021; 13(4): 1149. CrossRef - Analysis of the relationship between periodontitis and osteoporosis/fractures: a cross-sectional study
Seok-Jin Hong, Byoung-Eun Yang, Dae-Myoung Yoo, Sung-Jae Kim, Hyo-Geun Choi, Soo-Hwan Byun
BMC Oral Health.2021;[Epub] CrossRef - Effect of Dosing Interval on Compliance of Osteoporosis Patients on Bisphosphonate Therapy: Observational Study Using Nationwide Insurance Claims Data
Hyunil Lee, Sangcheol Lee, Dokyung Kim, Weonmin Cho, Sungtan Cho, Siyeong Yoon, Soonchul Lee
Journal of Clinical Medicine.2021; 10(19): 4350. CrossRef - Effects of a health-belief-model-based osteoporosis- and fall-prevention program on women at early old age
Sukhee Ahn, Jiwon Oh
Applied Nursing Research.2021; 59: 151430. CrossRef - Analyses of the relationship between hyperuricemia and osteoporosis
Jung Woo Lee, Bong Cheol Kwon, Hyo Geun Choi
Scientific Reports.2021;[Epub] CrossRef - Analysis of Anthropometric and Behavioral Factors of Korean Female Adolescents According to Age of Menarche: 2013~2017 Korea National Health and Nutrition Examination Survey
Eun–Joo Jeong, Bok-Mi Jung
The Korean Journal of Community Living Science.2020; 31(3): 393. CrossRef - What are the illnesses associated with frailty in community-dwelling older adults: the Korean Frailty and Aging Cohort Study
Sunyoung Kim, Hee-Won Jung, Chang Won Won
The Korean Journal of Internal Medicine.2020; 35(4): 1004. CrossRef - Factors Influencing on Health-Related Quality of Life among Men Osteoporosis Patients over 50 Years
Ji Young Kim, Youngran Yang
Korean Journal of Adult Nursing.2020; 32(2): 145. CrossRef - Bone health-promoting bioactive peptides
Chang-Bum Ahn, Jae-Young Je
Journal of Food Biochemistry.2019; 43(1): e12529. CrossRef - Associations of obesity with osteoporosis and metabolic syndrome in Korean postmenopausal women: a cross-sectional study using national survey data
Hyun-Young Kim, Yunmi Kim
Archives of Osteoporosis.2019;[Epub] CrossRef - Association between Metabolic Syndrome and Osteoporosis in Korean Adults Aged Over 50 Years Old Using the Korea National Health and Nutrition Examination Survey, 2016-2017
Hyeon Hwa Lee, Mi Ah Han, Jong Park
Journal of Health Informatics and Statistics.2019; 44(3): 245. CrossRef - The Relationship of Neutrophil-Lymphocyte Ratio and Platelet-Lymphocyte Ratio with Bone Mineral Density in Korean Postmenopausal Women
San-Hui Lee, So-Yeon Ryu, Jong Park, Min-Ho Shin, Mi-Ah Han, Seong-Woo Choi
Chonnam Medical Journal.2019; 55(3): 150. CrossRef - Gender differences in anti-osteoporosis drug treatment after osteoporotic fractures
Youn Jung, Yeonhee Ko, Ha Young Kim, Yong Chan Ha, Young-Kyun Lee, Tae-Young Kim, Dong-soo Choo, Sunmee Jang
Journal of Bone and Mineral Metabolism.2019; 37(1): 134. CrossRef - Effect of duration of diabetes on bone mineral density: a population study on East Asian males
Miso Jang, Hyunkyung Kim, Shorry Lea, Sohee Oh, Jong Seung Kim, Bumjo Oh
BMC Endocrine Disorders.2018;[Epub] CrossRef - Risk Factors for Unawareness of Obstructive Airflow Limitation among Adults with Chronic Obstructive Pulmonary Disease
Mirae Jo, Heeyoung Oh
Journal of Korean Academy of Community Health Nursing.2018; 29(3): 290. CrossRef - Factors Influencing Hemodialysis Unit Nurses' Compliance with Standard Precautions using Hierarchical Linear Modeling
Miyeun Kim, Juhhyun Shin
Korean Journal of Adult Nursing.2018; 30(2): 161. CrossRef - Contingent association between the size of the social support network and osteoporosis among Korean elderly women
Seungwon Lee, Da Hea Seo, Kyoung Min Kim, Eun Young Lee, Hyeon Chang Kim, Chang Oh Kim, Yoosik Youm, Yumie Rhee, Dengshun Miao
PLOS ONE.2017; 12(7): e0180017. CrossRef - Associations Between Reported Dietary Sodium Intake and Osteoporosis in Korean Postmenopausal Women: The 2008-2011 Korea National Health and Nutrition Examination Survey
Yunmi Kim, Hyun-Young Kim, Jung Hwan Kim
Asia Pacific Journal of Public Health.2017; 29(5): 430. CrossRef - Comparison in Adherence to Osteoporosis Guidelines according to Bone Health Status in Korean Adult
Hee-Sook Lim, Soon-Kyung Kim, Hae-Hyeog Lee, Dong Won Byun, Yoon-Hyung Park, Tae-Hee Kim
Journal of Bone Metabolism.2016; 23(3): 143. CrossRef - Influencing Factors on Osteopenia and Osteoporosis in Korean Aged 50 Years and Above
Eun Young Jeon, Sook Young Kim
The Korean Journal of Rehabilitation Nursing.2016; 19(2): 148. CrossRef - Incidence Rates of Osteopenia Based on the Appendicular Muscle Mass in the Elderly Korean Males
Yonghwan Kim, Haemi Jee
Exercise Science.2016; 25(3): 189. CrossRef - Association of Sarcopenia and Physical Activity with Femur Bone Mineral Density in Elderly Women
Inhwan Lee, Changduk Ha, Hyunsik Kang
Journal of Exercise Nutrition & Biochemistry.2016; 20(1): 23. CrossRef
- Evaluation of radiation dose to Korean population by general radiography
- 2,459 View
- 10 Download
- 32 Crossref
- Update on Irritable Bowel Syndrome Program of Research
- Margaret Heitkemper, Monica Jarrett, Sang-Eun Jun
- J Korean Acad Nurs 2013;43(5):579-586. Published online October 31, 2013
- DOI: https://doi.org/10.4040/jkan.2013.43.5.579
-
Abstract
PDF
Purpose This article provides an update and overview of a nursing research program focused on understanding the pathophysiology and management of irritable bowel syndrome (IBS).
Methods This review includes English language papers from the United States, Europe, and Asia (e.g., South Korea) from 1999 to 2013. We addressed IBS as a health problem, emerging etiologies, diagnostic and treatment approaches and the importance of a biopsychosocial model.
Results IBS is a chronic, functional gastrointestinal disorder characterized by recurrent episodes of abdominal pain and alterations in bowel habit (diarrhea, constipation, mixed). It is a condition for which adults, particularly women ages 20-45, seek health care services in both the United States and South Korea. Clinically, nurses play key roles in symptom prevention and management including designing and implementing approaches to enhance the patients' self-management strategies. Multiple mechanisms are believed to participate in the development and maintenance of IBS symptoms including autonomic nervous system dysregulation, intestinal inflammation, intestinal dysbiosis, dietary intolerances, alterations in emotion regulation, heightened visceral pain sensitivity, hypothalamic-pituitary-adrenal dysregulation, and dysmotility. Because IBS tends to occur in families, genetic factors may also contribute to the pathophysiology. Patients with IBS often report a number of co-morbid disorders and/or symptoms including poor sleep.
Conclusion The key to planning effective management strategies is to understand the heterogeneity of this disorder. Interventions for IBS include non-pharmacological strategies such as cognitive behavior therapy, relaxation strategies, and exclusion diets.
-
Citations
Citations to this article as recorded by- The effects of vitamin D intake and status on symptom severity and quality-of-life in adults with irritable bowel syndrome (IBS): a systematic review and meta-analysis
Kelly C. Cara, Salima F. Taylor, Haya F. Alhmly, Taylor C. Wallace
Critical Reviews in Food Science and Nutrition.2025; 65(25): 4994. CrossRef - Irritable bowel syndrome: neurological aspects of pathogenesis and therapy
F. A. Yusupov, I. T. Ydyrysov, A. A. Yuldashev
Experimental and Clinical Gastroenterology.2024; (11): 128. CrossRef - The role of intestinal microbiota on pre-eclampsia: Systematic review and meta-analysis
Tamy Colonetti, Diandra Limas Carmo Teixeira, Antonio José Grande, Maria Laura Rodrigues Uggioni, Jaqueline Generoso, Seeromanie Harding, Ana Rodriguez-Mateos, Peterson Rech, Fabio Rosa Silva, Indianara Toreti, Luciane Ceretta, Maria Inês Rosa
European Journal of Obstetrics & Gynecology and Reproductive Biology.2023; 291: 49. CrossRef - Golden bifid might improve diarrhea-predominant irritable bowel syndrome via microbiota modulation
Mei Luo, Qin Liu, Lin Xiao, Li-Shou Xiong
Journal of Health, Population and Nutrition.2022;[Epub] CrossRef - A Microbial Relationship Between Irritable Bowel Syndrome and Depressive Symptoms
Nicole B. Perez, Fay Wright, Allison Vorderstrasse
Biological Research For Nursing.2021; 23(1): 50. CrossRef - Dysbiosis of the Gut Microbiome: A Concept Analysis
Nicole B. Perez, Caroline Dorsen, Allison Squires
Journal of Holistic Nursing.2020; 38(2): 223. CrossRef - Irritable bowel syndrome and small intestinal bacterial overgrowth: Assessment with breath test
LA Costa, TNF Gomes, CU Braga, L Lenz, SJ Miszputen, O Ambrogini
Archives of Clinical Gastroenterology.2020; : 041. CrossRef - Yoga for Teens With Irritable Bowel Syndrome
Subhadra Evans, Laura C. Seidman, Kirsten Lung, Beth Sternlieb, Lonnie K. Zeltzer
Holistic Nursing Practice.2018; 32(5): 253. CrossRef - Prevalence and Factors related to Irritable Bowel Syndrome in University Students
Jin-Hee Park, Young-Mi Jung, Hye Jin Lee, Ji-Young Seo
Journal of Korean Academy of Fundamentals of Nursing.2018; 25(4): 282. CrossRef - Irritable Bowel Syndrome
Kristen Ronn Weaver, Gail D'Eramo Melkus, Wendy A. Henderson
AJN, American Journal of Nursing.2017; 117(6): 48. CrossRef - Arabinogalactan and fructooligosaccharides improve the gut barrier function in distinct areas of the colon in the Simulator of the Human Intestinal Microbial Ecosystem
David Daguet, Iris Pinheiro, An Verhelst, Sam Possemiers, Massimo Marzorati
Journal of Functional Foods.2016; 20: 369. CrossRef - Efficacy and Safety of High Specific Volume Polysaccharide—A New Type of Dietary Fiber for Treatment of Functional Constipation and IBS-C
Liang CONG, Jing-Ting MA, Zhen-Jing JIN, Li-Wei DUAN, Wei-Ping SU, Jing ZHENG, Ling-Juan ZHANG, Jia XU, Dong-Fu LI
Journal of Nutritional Science and Vitaminology.2015; 61(4): 326. CrossRef - Tong Xie Yao Fang relieves irritable bowel syndrome in ratsviamechanisms involving regulation of 5-hydroxytryptamine and substance P
Yue Yin, Lei Zhong, Jian-Wei Wang, Xue-Ying Zhao, Wen-Jing Zhao, Hai-Xue Kuang
World Journal of Gastroenterology.2015; 21(15): 4536. CrossRef - Aspects of the non-pharmacological treatment of irritable bowel syndrome
Elsa Maria Eriksson
World Journal of Gastroenterology.2015; 21(40): 11439. CrossRef - Early Adverse Life Events and Resting State Neural Networks in Patients With Chronic Abdominal Pain
Arpana Gupta, Lisa Kilpatrick, Jennifer Labus, Kirsten Tillisch, Adam Braun, Jui-Yang Hong, Cody Ashe-McNalley, Bruce Naliboff, Emeran A. Mayer
Psychosomatic Medicine.2014; 76(6): 404. CrossRef - So-Eum Type as an Independent Risk Factor for Irritable Bowel Syndrome: A Population-Based Study in Korea
Seung Ku Lee, Dae Wui Yoon, Hyeryeon Yi, Si Woo Lee, Jong Yeol Kim, Jin Kwan Kim, Jeong Hwa Hong, Chol Shin
The Journal of Alternative and Complementary Medicine.2014; 20(11): 846. CrossRef
- The effects of vitamin D intake and status on symptom severity and quality-of-life in adults with irritable bowel syndrome (IBS): a systematic review and meta-analysis
- 2,052 View
- 6 Download
- 16 Crossref
- Meta-Analysis of Spiritual Intervention Studies on Biological, Psychological, and Spiritual Outcomes
- Pok-Ja Oh, Young-Hyun Kim
- J Korean Acad Nurs 2012;42(6):833-842. Published online December 31, 2012
- DOI: https://doi.org/10.4040/jkan.2012.42.6.833
-
Abstract
PDF
Purpose The purpose of this study was to evaluate the effectiveness of spiritual intervention studies by examining biological, psychological, and spiritual outcomes.
Methods From electronic databases 2522 studies were retrieved, of which 21 studies met the inclusion criteria. These studies had 1411 participants. Two authors independently extracted data from the selected studies and assessed the methodological quality. The data were analyzed using the RevMan 5.1 program of the Cochrane library.
Results Overall effect size of spiritual intervention on spiritual and psychological (depression and anxiety) outcomes were moderate (d=-0.65 to d=-0.76,
p <.001). The effects on biological outcomes (pain and functional status) ranged from -0.51 to -0.39, respectively. No publication bias was detected as evaluated by a funnel plot. Spiritual intervention had a moderate effect on psychological and spiritual outcomes and a smaller effect on biological outcomes.Conclusion The results of this study suggest that spiritual intervention can relieve depression and anxiety. Further randomized controlled trials studies are needed to evaluate the effects of spiritual intervention on biological outcomes.
-
Citations
Citations to this article as recorded by- Effectiveness of Interventions on Death Anxiety and Fear in Adults with Chronic Disease: A Systematic Review and Meta-Analysis of Randomized Controlled Trials
Merve Gulbahar Eren, Kübra Üçgül, Havva Sert
OMEGA - Journal of Death and Dying.2025; 91(4): 2007. CrossRef - Effects of counselling and spiritual care program on anxiety in patients with chronic diseases: A systematic review and meta-analysis
Nader Salari, Mohsen Kazeminia, Alireza Abdi, Amir Abdolmaleki, Nasrin Abdoli, Masoud Mohammadi, Shamarina Shohaimi
Current Psychology.2023; 42(12): 9943. CrossRef - The development of a Cancer Pain Belief Modification Program for patients with oral cancer in China: a feasibility study
Rongna Wang, Xiaoyan Zheng, Xixi Su, Xiuyu Huang, Huangju Liu, Yulai Guo, Ji Gao
BMC Nursing.2023;[Epub] CrossRef - The Effects of Spiritual Well-being on Self-care Practices in People Undergoing Hemodialysis: The Mediating Effect of Hope
Bu Kyung Kim, Pok-Ja Oh
Korean Journal of Adult Nursing.2022; 34(6): 592. CrossRef - Abriendo nuevas puertas: Relevancia clínica de integrar la religión y la espiritualidad en la disciplina de la psicología
Orlando M. Pagan-Torres Ponce
Revista Puertorriqueña de Psicologia.2022; 33(2): 258. CrossRef - The Mediating Effect of Depression on the Relationship between Social Support, Spirituality and Burnout in Family Members of Patients with Cancer
Won-Hee Jun, Kyung-Sook Cha, Kee-Lyong Lee
International Journal of Environmental Research and Public Health.2021; 18(4): 1727. CrossRef - Spirituality, religiousness, and mental health: A review of the current scientific evidence
Giancarlo Lucchetti, Harold G Koenig, Alessandra Lamas Granero Lucchetti
World Journal of Clinical Cases.2021; 9(26): 7620. CrossRef - Analysis of Spiritual Care Experiences of Acute-Care Hospital Nurses
Ga Eon Lee, KyoungMi Kim
The Korean Journal of Hospice and Palliative Care.2020; 23(2): 44. CrossRef - The Effect of Religion Intervention on Life Satisfaction and Depression in Elderly with Heart Failure
Alireza Abdi, Askar Soufinia, Milad Borji, Asma Tarjoman
Journal of Religion and Health.2019; 58(3): 823. CrossRef - Initial Assessment and Care Planning in Palliative Hospice Care: Focus on Assessment Tools
Eun Ju Park, Su Jin Koh, Jae Kyung Cheon
The Korean Journal of Hospice and Palliative Care.2019; 22(2): 67. CrossRef - Experience of Cancer Patients Receiving Spiritual Nursing Care in one Christian General Hospital
Eun Youngi Seo, Suhye Kwon, Youngkyoung Kim, ALeum Han
Asian Oncology Nursing.2019; 19(3): 179. CrossRef - Complementary religious and spiritual interventions in physical health and quality of life: A systematic review of randomized controlled clinical trials
Juliane Piasseschi de Bernardin Gonçalves, Giancarlo Lucchetti, Paulo Rossi Menezes, Homero Vallada, Gianni Virgili
PLOS ONE.2017; 12(10): e0186539. CrossRef - Panorama das pesquisas em ciência, saúde e espiritualidade
Alexander Moreira-Almeida, Giancarlo Lucchetti
Ciência e Cultura.2016; 68(1): 54. CrossRef - Spirituality is associated with better prostate cancer treatment decision making experiences
Michelle A. Mollica, Willie Underwood, Gregory G. Homish, D. Lynn Homish, Heather Orom
Journal of Behavioral Medicine.2016; 39(1): 161. CrossRef - Validity and Reliability of Korean Version of the Spiritual Care Competence Scale
Mi Ja Chung, Youngrye Park, Young Eun
Journal of Korean Academy of Nursing.2016; 46(6): 871. CrossRef - Influence of Self-esteem, Empathy and Existential Well-being on Spiritual Care Competence in Nursing Students
Jin Kim, Sookyung Choi
Journal of Korean Academy of Fundamentals of Nursing.2015; 22(3): 328. CrossRef - Religious and spiritual interventions in mental health care: a systematic review and meta-analysis of randomized controlled clinical trials
J. P. B. Gonçalves, G. Lucchetti, P. R. Menezes, H. Vallada
Psychological Medicine.2015; 45(14): 2937. CrossRef - The Effects of Spiritual Interventions in Patients With Cancer: A Meta-Analysis
Pok-Ja Oh, Soo Hyun Kim
Oncology Nursing Forum.2014; 41(5): E290. CrossRef - Association between Spiritual Well-Being and Pain, Anxiety and Depression in Terminal Cancer Patients: A Pilot Study
Yong Joo Lee, Chul-Min Kim, John A. Linton, Duk Chul Lee, Sang-Yeon Suh, Ah-Ram Seo, Hong-Yup Ahn
The Korean Journal of Hospice and Palliative Care.2013; 16(3): 175. CrossRef - Meta-analysis of Psychosocial Interventions to Reduce Pain in Patients with Cancer
Pok Ja Oh, Suk Jung Han
Journal of Korean Academy of Nursing.2013; 43(5): 658. CrossRef - Effect of Intervention Programs for Improving Maternal Adaptation in Korea: Systematic Review
Hee Sun Kang, Soo Young Yeom, Eun-Young Jun
Korean Journal of Women Health Nursing.2013; 19(3): 153. CrossRef
- Effectiveness of Interventions on Death Anxiety and Fear in Adults with Chronic Disease: A Systematic Review and Meta-Analysis of Randomized Controlled Trials
- 1,630 View
- 9 Download
- 21 Crossref
 First
First Prev
Prev

