 Submit an article
Submit an article
Search
- Page Path
- HOME > Search
Research Paper
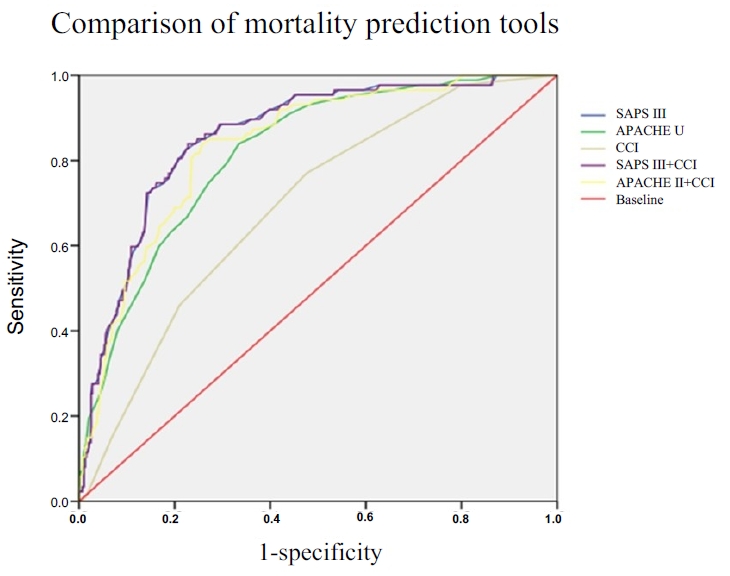
- Usefulness of Charlson comorbidity index-adjusted mortality prediction tools and factors influencing mortality in intensive care unit patients: a retrospective medical record review–based study
- Jai Jung Lee, Dong Yeon Kim, Min Ji Lee, Ji Young Kim
- J Korean Acad Nurs 2026;56(1):27-38. Published online February 11, 2026
- DOI: https://doi.org/10.4040/jkan.25094
-
 Abstract
Abstract
 PDF
PDF ePub
ePub - Purpose
This study aimed to estimate the mortality rate in adult intensive care units (ICUs) using the Charlson comorbidity index (CCI)-adjusted Acute Physiology and Chronic Health Evaluation (APACHE) II and Simplified Acute Physiology Score (SAPS) III models, and to identify factors influencing mortality.
Methods
This retrospective cohort study included adult patients admitted to the ICU at a tertiary hospital between June 1 and August 31, 2022. Among the 1,098 screened patients, those younger than 18 years, those discharged within 48 hours, and those with missing medical records were excluded. In total, 482 patients were analyzed using the chi-square test, independent t-test, and multivariate logistic regression. Model performance was evaluated using the c-statistic and the Hosmer-Lemeshow goodness-of-fit test.
Results
The predictive accuracy of the mortality models was shown by c-statistic values of 0.817 for APACHE II, 0.857 for SAPS III, 0.697 for CCI, and 0.834 for CCI-adjusted APACHE II (0.834). Mechanical ventilation, cardiopulmonary cerebral resuscitation, continuous renal replacement therapy, and the presence of leukemia or lymphoma were significant predictors of mortality in adult ICU patients. Among the evaluated models, SAPS III and CCI-adjusted APACHE II demonstrated the highest predictive power.
Conclusion
The findings indicate that incorporating comorbidity indices such as the CCI with acute physiological parameters improves the accuracy of mortality prediction in ICU patients. Understanding mortality prediction models is essential for nurses to provide individualized, evidence-based, and high-quality care in adult ICUs.
- 2,740 View
- 236 Download

Original Articles
- Evaluating the Validity of the Pediatric Index of Mortality II in the Intensive Care Units
- Jung Soon Kim, Sun Joo Boo
- Journal of Korean Academy of Nursing 2005;35(1):47-55. Published online March 28, 2017
- DOI: https://doi.org/10.4040/jkan.2005.35.1.47
-
Abstract
PDF
Purpose This study was to evaluate the validity of the Pediatric Index of Mortality II(PIM II).
Method The first values on PIM II variables following ICU admission were collected from the patient's charts of 548 admissions retrospectively in three ICUs(medical, surgical, and neurosurgical) at P University Hospital and a cardiac ICU at D University Hospital in Busan from January 1, 2002 to December 31, 2003. Data was analyzed with the SPSSWIN 10.0 program for the descriptive statistics, correlation coefficient, standardized mortality ratio(SMR), validity index(sensitivity, specificity, positive predictive value, negative predictive value), and AUC of ROC curve.
Result The mortality rate was 10.9%(60 cases) and the predicted death rate was 9.5%. The correlation coefficient(r) between observed and expected death rates was .929(p<.01) and SMR was 1.15. Se, Sp, pPv, nPv, and the correct classification rate were .80, .96, .70, .98, and 94.0% respectively. In addition, areas under the curve(AUC) of the receiver operating characteristic(ROC) was 0.954(95% CI=0.919~0.989). According to demographic characteristics, mortality was underestimated in the medical group and overestimated in the surgical group. In addition, the AUCs of ROC curve were generally high in all subgroups.
Conclusion The PIM II showed a good, so it can be utilized for the subject hospital.
-
Citations
Citations to this article as recorded by
- The Values of the Pediatric Logistic Organ Dysfunction (PELOD) Score and the Pediatric Index of Mortality (PIM) 2 Score in Emergency Department and Intensive Care Unit
Si Kyoung Jeong, Woon Jeong Lee, Yun Joo Moon, Seon Hee Woo, Yeon Young Kyong, Se Min Choi, Won Jung Jeong, Kyu Nam Park
The Korean Journal of Critical Care Medicine.2010; 25(3): 144. CrossRef - Outcome and risk factors of pediatric hemato-oncology patients admitted in pediatric intensive care unit
Bo Eun Kim, Eun Ju Ha, Keun Wook Bae, Seonguk Kim, Ho Joon Im, Jong Jin Seo, Seong Jong Park
Korean Journal of Pediatrics.2009; 52(10): 1153. CrossRef - Performance effectiveness of pediatric index of mortality 2 (PIM2) and pediatricrisk of mortality III (PRISM III) in pediatric patients with intensive care in single institution: Retrospective study
Hui Seung Hwang, Na Young Lee, Seung Beom Han, Ga Young Kwak, Soo Young Lee, Seung Yun Chung, Jin Han Kang, Dae Chul Jeong
Korean Journal of Pediatrics.2008; 51(11): 1158. CrossRef
- The Values of the Pediatric Logistic Organ Dysfunction (PELOD) Score and the Pediatric Index of Mortality (PIM) 2 Score in Emergency Department and Intensive Care Unit
- 1,040 View
- 0 Download
- 3 Crossref
- Pre- and In-Hospital Delay in Treatment and in-Hospital Mortality after Acute Myocardial Infarction
- Kyuneh An, Bongyeun Koh
- Journal of Korean Academy of Nursing 2003;33(8):1153-1160. Published online March 28, 2017
- DOI: https://doi.org/10.4040/jkan.2003.33.8.1153
-
Abstract
PDF
Purpose 1) To identify the time taken from symptom onset to the arrival at the hospital (pre-hospital delay time) and time taken from the arrival at the hospital to the initiation of the major treatment (in-hospital delay time) 2) to examine whether rapid treatment results in lower mortality. 3) to examine whether the pre- and in-hospital delay time can independently predict in-hospital mortality.
Methods A retrospective study with 586 consecutive AMI patients was conducted.
Results Pre-hospital delay time was 5.25 (SD=10.36), and in-hospital delay time was 1.10 (SD=1.00) hours for the thrombolytic therapy and 50.24 (SD=121.18) hours for the percutaneous transluminal coronary angioplasty(PTCA). In-hospital mortality was the highest when the patients were treated between 4 to 48 hours after symptom onset using PTCA (rho=.02), and when treated between 30 minutes and one hour after hospital arrival using thrombolytics (rho=.01). Using a hierarchical logistic regression model, the pre- and in-hospital delay times did not predict the in-hospital mortality.
Conclusion Pre- and in-hospital delay times need to be decreased to meet the desirable therapeutic time window. Thrombolytics should be given within 30 minutes after arrival at the hospital, and PTCA should be initiated within 4 hours after symptom onset to minimize in-hospital mortality of AMI patients.
-
Citations
Citations to this article as recorded by- Comparison of Clinical Manifestations and Treatment-Seeking Behavior in Younger and Older Patients with First-time Acute Coronary Syndrome
Seon Young Hwang
Journal of Korean Academy of Nursing.2009; 39(6): 888. CrossRef
- Comparison of Clinical Manifestations and Treatment-Seeking Behavior in Younger and Older Patients with First-time Acute Coronary Syndrome
- 971 View
- 3 Download
- 1 Crossref
- Accidental Mortality and Compensation Payment in School Activities among Elementary, Middle and High School Students in Seoul over Twenty Years (1988-2007)
- Sun Mi Shin, Hee Woo Lee
- J Korean Acad Nurs 2012;42(2):248-257. Published online April 30, 2012
- DOI: https://doi.org/10.4040/jkan.2012.42.2.248
-
Abstract
PDF
Purpose The purpose of this study was to identify accidental mortality during school activities of students in elementary, middle or high school in Seoul and consequent compensation payment.
Methods Fifty-eight students died due to accidents during the period 1988 through 2007. Data were obtained from the Seoul School Safety and Insurance Association, and Seoul Metropolitan Office of Education. Chi-square, t test, and ANCOVA were used in the data analysis.
Results Among students, 75.9% were male and 37.9% were high school students. Accidental mortality was 1.61 per one million students (2.33 for male, and 0.82 for female students, and 0.93, 2.13 and 2.31 for elementary, middle and high school students, respectively). Mortality caused by drowning and falls per one million student was 0.85 and 0.74 for male, and 0.23 and 0.35 for female students. After age, year and cause were adjusted using ANCOVA, the mean compensation payment was 40,615 thousand won for male, and 62,000 thousands for female students. Highest compensation payment was 127,137 thousand for cerebral concussion after age, gender, year and cause were adjusted.
Conclusion To decrease student accidental mortality, especially drowning and falls, development of efficient safety-enforcing education is essential to prevent injuries and avoid preventable compensation costs.
- 1,254 View
- 0 Download
- A Systematic Review of Psychological Distress as a Risk Factor for Recurrent Cardiac Events in Patients with Coronary Artery Disease
- Jin-Hee Park, Sun Hyoung Bae
- J Korean Acad Nurs 2011;41(5):704-714. Published online October 31, 2011
- DOI: https://doi.org/10.4040/jkan.2011.41.5.704
-
Abstract
PDF
Purpose The purpose of this study was to determine whether psychological distress is an independent risk factor for recurrent cardiac events in patients with coronary artery disease (CAD).
Methods A prospective cohort of studies that measured psychological distress and the incidence of recurrent cardiac events in the adult population were included. Three computerized databases were assessed (PubMed, CINAHL, and PSYCINFO). Meta-analysis was conducted using a random-effects model to determine summary estimates of risks of major recurrent cardiac events associated with each psychological distress. Of 506 publications identified, 33 met inclusion criteria, and 24 studies were used to estimate effect size of psychological distress on recurrent cardiac events.
Results Mean number in the research sample was 736 and mean time of follow-up was 4.0 years. Depression, anxiety, anger, and hostility as psychological factors were studied. According to estimation of effect size using random model effect, depression (OR=1.39, 95% CI: 1.22-1.57), anxiety (OR=1.22, 95% CI: 0.96-1.56), and anger/hostility (OR=1.29, 95% CI: 1.07-1.57) CAD patients in significantly increased risk for recurrent cardiac events.
Conclusion Finding suggests that psychological distress in forms of depression, anxiety, anger, and hostility impact unfavorably on recurrent cardiac events in CAD patients.
-
Citations
Citations to this article as recorded by- NAMS task force report on mental stress
Rajesh Sagar, Kaushik Chatterjee, Sandeep Thareja, Anurag Timothy, A.S. Yadav, Prateek Yadav, Rajinder Dhamija, S.V. Madhu, Preethy Kathiresan, Pratibha Prasad, Swati Kedia Gupta, Kalpana Srivastava
Annals of the National Academy of Medical Sciences (India).2025; 61: 66. CrossRef - Impact of Type D Personality and Health Literacy on Resilience of Inpatients with Cardiovascular Diseases: A Cross-Sectional Study
Da Eun Kim, Seon Young Hwang
Korean Journal of Adult Nursing.2023; 35(1): 23. CrossRef - The Effect of Perceived Stress, Fine Dust Risk Perception, and Resilience on Stress Response in Patients with Respiratory and Circulatory Disorders
Jin-Hee Park, Kuem-Sun Han
STRESS.2021; 29(1): 21. CrossRef - Associations of depression and anxiety with cardiovascular risk among people living with HIV/AIDS in Korea
Kyong Sil Park, Seon Young Hwang, Bo Youl Choi, June Kim, Sang Il Kim, Woo-Joo Kim, Chun Kang
Epidemiology and Health.2020; 43: e2021002. CrossRef - Impact of Type D Personality on Depression, Anxiety, and Health-related Quality of Life among Coronary Artery Disease Patients: A Systematic Review and Meta-analysis
Sun Hyoung Bae, Jin-Hee Park
Korean Journal of Adult Nursing.2019; 31(3): 219. CrossRef - Analysis of the relationship between community characteristics and depression using geographically weighted regression
Hyungyun Choi, Ho Kim
Epidemiology and Health.2017; 39: e2017025. CrossRef - Influencing Effects of Type D Personality on Symptom Experiences and Quality of Life in Patients with Percutaneous Coronary Intervention
Eun Hee Jo, Sun Hee Han, Myung Ha Lee, Sung Reul Kim
Korean Journal of Adult Nursing.2016; 28(5): 536. CrossRef - Depression and Anxiety as Predictors of Recurrent Cardiac Events 12 Months After Percutaneous Coronary Interventions
Jin-Hee Park, Seung-Jea Tahk, Sun Hyoung Bae
Journal of Cardiovascular Nursing.2015; 30(4): 351. CrossRef - Anger, anger expression, cardiovascular risk factors, and gastrointestinal symptoms by hwa-byung symptoms in Korean adult women
Young-Joo Park, Sook-Ja Lee, Nah-Mee Shin, Hyunjeong Shin, Hyun Cheol Kang, Yoon Tae Jin, Song I. Jeon, Inhae Cho
Applied Nursing Research.2015; 28(4): 398. CrossRef - Risk Factor–tailored Small Group Education for Patients with First-time Acute Coronary Syndrome
Seon Young Hwang, Jin Shil Kim
Asian Nursing Research.2015; 9(4): 291. CrossRef - Influences of Knowledge, Self-efficacy, and Social Support on Sick Role Behavior in Patients with Coronary Artery Disease
Soonhee Kim, Sunhee Lee
Journal of Korean Public Health Nursing.2014; 28(2): 228. CrossRef - Factors Influencing the Quality of Life in Low- Income Elders Living at Home: A Literature Review
Chung-Min Cho
Journal of Korean Public Health Nursing.2013; 27(2): 372. CrossRef - Effects of a psychoeducational intervention for secondary prevention in Korean patients with coronary artery disease: A pilot study
Jin‐Hee Park, Seung‐Jae Tahk, Sun Hyoung Bae, Youn‐Jung Son
International Journal of Nursing Practice.2013; 19(3): 295. CrossRef - Stress and cardiovascular disease
Jung Jin Cho
Journal of the Korean Medical Association.2013; 56(6): 462. CrossRef
- NAMS task force report on mental stress
- 1,868 View
- 18 Download
- 14 Crossref
- Verification of Validity of MPM II for Neurological Patients in Intensive Care Units
- Heejeong Kim, Kyunghee Kim
- J Korean Acad Nurs 2011;41(1):92-100. Published online February 28, 2011
- DOI: https://doi.org/10.4040/jkan.2011.41.1.92
-
Abstract
PDF
Purpose Mortality Provability Model (MPM) II is a model for predicting mortality probability of patients admitted to ICU. This study was done to test the validity of MPM II for critically ill neurological patients and to determine applicability of MPM II in predicting mortality of neurological ICU patients.
Methods Data were collected from medical records of 187 neurological patients over 18 yr of age who were admitted to the ICU of C University Hospital during the period from January 2008 to May 2009. Collected data were analyzed through χ2 test, t-test, Mann-Whiteny test, goodness of fit test, and ROC curve.
Results As to mortality according to patients' general and clinically related characteristics, mortality was statistically significantly different for ICU stay, hospital stay, APACHE III score, APACHE predicted death rate, GCS, endotracheal intubation, and central venous catheter. Results of Hosmer-Lemeshow goodness-of-fit test were MPM II0 (χ2=0.02,
p =.989), MPM II24 (χ2=0.99p =.805), MPM II48 (χ2=0.91,p =.822), and MPM II72 (χ2=1.57,p =.457), and results of the discrimination test using the ROC curve were MPM II0, .726 (p <.001), MPM II24, .764 (p <.001), MPM II48, .762 (p <.001), and MPM II72, .809 (p <.001).Conclusion MPM II was found to be a valid mortality prediction model for neurological ICU patients.
-
Citations
Citations to this article as recorded by- Usefulness of Charlson comorbidity index-adjusted mortality prediction tools and factors influencing mortality in intensive care unit patients: a retrospective medical record review–based study
Jai Jung Lee, Dong Yeon Kim, Min Ji Lee, Ji Young Kim
Journal of Korean Academy of Nursing.2026; 56(1): 27. CrossRef - Development of a patient classification system for critical care nursing based on nursing intensity
Yukyung Ko, Bohyun Park, Hanju Lee, Donghwan Kim
International Journal of Nursing Practice.2023;[Epub] CrossRef - Validation Study of the Estimated Glycemic Load Model Using Commercially Available Fast Foods
Miran Lee, Haejin Kang, Sang-Jin Chung, Kisun Nam, Yoo Kyoung Park
Frontiers in Nutrition.2022;[Epub] CrossRef - Comparison of acute physiology and chronic health evaluation II and Glasgow Coma Score in predicting the outcomes of Post Anesthesia Care Unit's patients
Mohammad Hosseini, Jamileh Ramazani
Saudi Journal of Anaesthesia.2015; 9(2): 136. CrossRef - Evaluation of Critical Patient Severity Classification System(CPSCS) for neurocritical patients in intensive unit
Hee-Jeonh Kim
Journal of the Korea Academia-Industrial cooperation Society.2012; 13(11): 5238. CrossRef
- Usefulness of Charlson comorbidity index-adjusted mortality prediction tools and factors influencing mortality in intensive care unit patients: a retrospective medical record review–based study
- 1,480 View
- 4 Download
- 5 Crossref
- A Study on Regional Differentials in Death Caused by Suicide in South Korea
- Eunok Park, Mi Yeol Hyun, Chang In Lee, Eun Joo Lee, Seong Chul Hong
- Journal of Korean Academy of Nursing 2007;37(1):44-51. Published online February 28, 2007
- DOI: https://doi.org/10.4040/jkan.2007.37.1.44
-
Abstract
PDF
Purpose The purpose of this study was to compare suicide mortality by region in South Korea.
Method Suicide mortality differentials were calculated for several mortality indicators by geographical regions from raw data of the cause of death from KNSO.
Results The results are as follows; the Crude suicide death rate was 22.63 per 100,000. The highest was in Kangwon showing 37.84% whereas, Chungnam, and Jeonbuk followed after. Suicide was 4.4% of all causes of death, but Inchon and Ulsan showed a higher proportion. The male suicide death rate was 31.12 per 100,000 and females 14.09. The ratio of gender suicide mortality was 2.21, per 100,000 and was the highest in Jeju. For age-specific suicide death rates, the rate increased as age advanced, showing 2.33 per 100,000 in 0-19years, 18.68 in 20-39, 30.48 in 40-59,63.33 in 60 years and over. In Ulsan, Kangwon, and Inchon, age-specific suicide death rates of the 60 and over age group were higher than other regions, Daegu, Busan, and Kangwon showed a higher age-specific suicide mortality of the 40-59 age group, and Kangwon, Jeonnam, and Chungnam had a higher age-specific suicide mortality of the 20-39 age group.
Conclusions Suicide mortality differed by region. These results can be used for a regional health care plan and planning for suicide prevention by regions.
-
Citations
Citations to this article as recorded by- Urban and rural differences in suicidal ideation and associated factors among older Koreans: Results from the Korean National Survey 2012–2013
Eunok Park, Hyo Young Lee
Current Psychology.2023; 42(9): 7002. CrossRef - Changes in the Suicide Rate of Older Adults According to Gender, Age, and Region in South Korea from 2010 to 2017
Kyu-Hyoung Jeong, Ji-Yeon Yoon, Seoyoon Lee, Sunghwan Cho, Hyun-Jae Woo, Sunghee Kim
Healthcare.2022; 10(11): 2333. CrossRef - Regional Disparities of Suicide Mortality by Gender
Eun-Won Seo, Jin-Mi Kwak, Da-Yang Kim, Kwang-Soo Lee
Health Policy and Management.2015; 25(4): 285. CrossRef - The Effect of the Regional Factors on the Variation of Suicide Rates: Geographic Information System Analysis Approach
Seong-Yong Park, Kwang-Soo Lee
Health Policy and Management.2014; 24(2): 143. CrossRef - The Psychiatric Treatment Link Characteristics of Suicide Attempters Visiting Emergency Room
Han Na Park, Seong-Sook Jun, Eun Kyung Byun
Journal of East-West Nursing Research.2014; 20(2): 93. CrossRef
- Urban and rural differences in suicidal ideation and associated factors among older Koreans: Results from the Korean National Survey 2012–2013
- 1,352 View
- 3 Download
- 5 Crossref
 First
First Prev
Prev

