 Submit an article
Submit an article
Articles
- Page Path
- HOME > J Korean Acad Nurs > Ahead-of print articles > Article
-
Research Paper
- Development of emergency nursing educational materials in Lao People's Democratic Republic: a methodological study
-
Jina Oh1
 , Eunsil Won1, Seohyun Won1, Sunmi Kim2, Seryung Oh3, Souksavanh Phanpaseuth4, Anousone Sisoulath4, Lamngeun Silavong5
, Eunsil Won1, Seohyun Won1, Sunmi Kim2, Seryung Oh3, Souksavanh Phanpaseuth4, Anousone Sisoulath4, Lamngeun Silavong5 -
DOI: https://doi.org/10.4040/jkan.25174
Published online: May 21, 2026
1College of Nursing, Inje University, Busan, South Korea
2International Educational Development Cooperation, Pusan National University, Busan, South Korea
3Industry Academic Cooperation Foundation, Inje University, Gimhae, South Korea
4Faculty of Nursing Sciences, University of Health Sciences, Vientiane, Lao PDR
5Nursing Division, Mahosot Hospital, Vientiane, Lao PDR
- Corresponding author: Eunsil Won College of Nursing, Inje University, 75 Bokji-ro, Busanjin-gu, Busan 47392, South Korea E-mail: woneunsil@naver.com
• Received: December 12, 2025 • Revised: April 28, 2026 • Accepted: April 28, 2026
© 2026 Korean Society of Nursing Science
This is an Open Access article distributed under the terms of the Creative Commons Attribution NoDerivs License (http://creativecommons.org/licenses/by-nd/4.0) If the original work is properly cited and retained without any modification or reproduction, it can be used and re-distributed in any format and medium.
- 28 Views
- 0 Download
Abstract
-
Purpose
- This study aimed to develop contextualized emergency nursing educational materials tailored to the Lao People’s Democratic Republic (Lao PDR). Emergency nurses in Lao PDR face challenges arising from the lack of standardized, culturally relevant learning resources. Existing materials are often adopted from other countries and do not adequately reflect local needs, contributing to inconsistencies in clinical practice. Developing locally tailored resources, supported by official development assistance, is therefore essential for improving emergency nursing education and practice.
-
Methods
- This study used a methodological design based on the Four-Door Model—Define, Design, Develop, and Disseminate—from 2021 to 2024. A situational analysis was conducted using a mixed-methods approach that included a quantitative survey of 70 nursing professionals and qualitative interviews with 52 stakeholders. Content validity and suitability were evaluated by a panel of six local experts using standardized validation forms and the Suitability Assessment of Materials (SAM).
-
Results
- Ten emergency nursing domains were developed to address both universal principles, including triage protocols and life support interventions, and Lao PDR-specific challenges. Validity and suitability were supported by a SAM score of 77.3%, indicating clinical accuracy and cultural appropriateness. The 269-page coursebook was distributed to partner nursing colleges, three central hospitals, and international organizations.
-
Conclusion
- This study developed the first comprehensive emergency nursing educational materials tailored to the Lao PDR context and written in the local language. These materials support continuing professional development and license renewal every 5 years. They also exemplify an international development paradigm that prioritizes recipient-country ownership and sustainable capacity building through collaborative knowledge creation.
Introduction
Methods
1) Define stage: Situational analysis
(1) Interviews for situational analysis
(2) Survey for situational analysis
2) Design stage: Core concept design and content organization
(1) Committee formation and operation
(2) Structuring core educational areas
3) Develop stage: Development of educational materials
(1) Content construction and drafting
(2) Validation and quality assessment
4) Disseminate stage: Finalization and dissemination
5) Ethical considerations
Results
1) Interviews for situational analysis
2) Survey for situational analysis
1) Committee formation and operation
2) Structuring core educational areas
1) Content construction and drafting
2) Validation and quality assessment
Discussion
Conclusion
-
Conflicts of Interest
No potential conflict of interest relevant to this article was reported.
-
Acknowledgements
None.
-
Funding
This study was supported by the Leading University Project for International Cooperation through the National Research Foundation of Korea (NRF) funded by the Ministry of Education (MOE) (grant number: 2020H1A7A2A02000042).
-
Data Sharing Statement
Please contact the corresponding author for data availability.
-
Supplementary Data
Supplementary data to this article can be found online at https://doi.org/10.4040/jkan.25174.
Supplementary Material 1.
-
Author Contributions
Conceptualization: JO, EW, SW. Data curation: JO, SK, SO, SP, AS, LS. Final approval of the manuscript: all authors. Formal analysis: JO, SK, SO, SP, AS, LS. Funding acquisition: JO. Investigation: SK, SO, SP, AS, LS. Methodology: JO, EW, SW. Project administration: JO, EW, SP, AS. Resources: SP, AS, LS. Software: SP, AS, LS. Supervision: JO, EW, SP, AS. Validation: JO, SP, AS, LS. Visualization: EW, SW. Writing–original draft: JO, EW, SW. Writing–review & editing: JO, EW, SW, SK, SO, SP, AS, LS.
Article Information
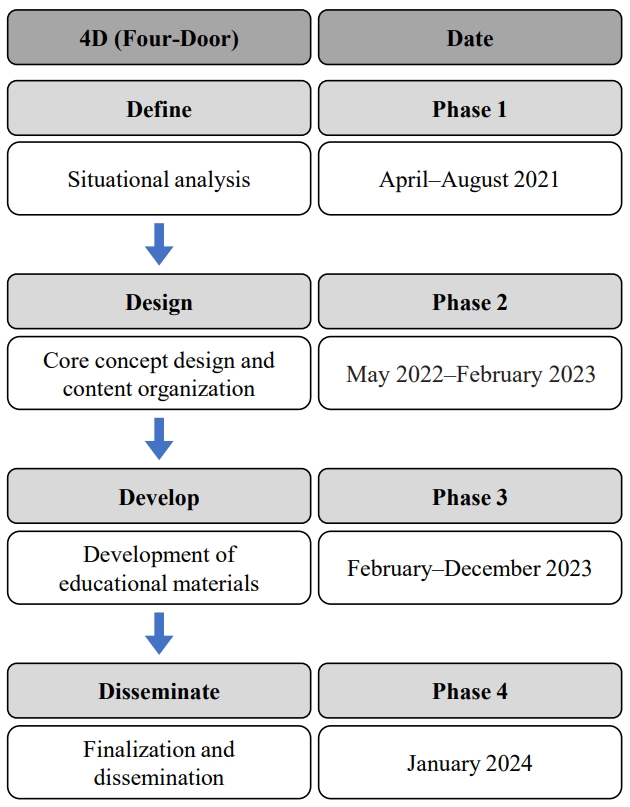
Table 1.Current status and problems of emergency nursing in hospitals in Lao PDR
Table 2.Priority knowledge and skill domains in emergency nursing (N=70)
Table 3.Initial framework of emergency nursing educational domains
Table 4.Final domains and contents of emergency nursing education materials
- 1. World Health Assembly. Emergency care systems for universal health coverage: ensuring timely care for the acutely ill and injured: WHA72.16. World Health Organization; 2019.
- 2. Anderson PD, Suter RE, Mulligan T, Bodiwala G, Razzak JA, Mock C, et al. World Health Assembly Resolution 60.22 and its importance as a health care policy tool for improving emergency care access and availability globally. Ann Emerg Med. 2012;60(1):35-44. https://doi.org/10.1016/j.annemergmed.2011.10.018ArticlePubMed
- 3. Lindström V, Falk AC. Emergency care nurses’ self-reported clinical competence before and after postgraduate education: a cross-sectional study. Int Emerg Nurs. 2023;70:101320. https://doi.org/10.1016/j.ienj.2023.101320ArticlePubMed
- 4. Hodgson NR, Kwun R, Gorbatkin C, Davies J, Fisher J; ACEP Emergency Medicine Practice Committee. Emergency department responses to nursing shortages. Int J Emerg Med. 2024;17(1):51. https://doi.org/10.1186/s12245-024-00628-yArticlePubMedPMC
- 5. Chang CY, Abujaber S, Reynolds TA, Camargo CA, Obermeyer Z. Burden of emergency conditions and emergency care usage: new estimates from 40 countries. Emerg Med J. 2016;33(11):794-800. https://doi.org/10.1136/emermed-2016-205709ArticlePubMedPMC
- 6. Goldsworthy S, Muir N, Baron S, Button D, Goodhand K, Hunter S, et al. The impact of virtual simulation on the recognition and response to the rapidly deteriorating patient among undergraduate nursing students. Nurse Educ Today. 2022;110:105264. https://doi.org/10.1016/j.nedt.2021.105264ArticlePubMed
- 7. Rybarczyk MM, Ludmer N, Broccoli MC, Kivlehan SM, Niescierenko M, Bisanzo M, et al. Emergency medicine training programs in low- and middle-income countries: a systematic review. Ann Glob Health. 2020;86(1):60. https://doi.org/10.5334/aogh.2681ArticlePubMedPMC
- 8. Damkliang J, Considine J, Kent B, Street M. Using an evidence-based care bundle to improve Thai emergency nurses’ knowledge of care for patients with severe traumatic brain injury. Nurse Educ Pract. 2015;15(4):284-292. https://doi.org/10.1016/j.nepr.2015.03.007ArticlePubMed
- 9. Subramanian P, Choy KL, Gobal SV, Mansor M, Ng KH. Impact of education on ventilator-associated pneumonia in the intensive care unit. Singapore Med J. 2013;54(5):281-284. https://doi.org/10.11622/smedj.2013109ArticlePubMed
- 10. World Health Organization. Global status report on road safety 2018. World Health Organization; 2019.
- 11. Whitaker J, Denning M, O’Donohoe N, Poenaru D, Guadagno E, Leather A, et al. Assessing trauma care health systems in low- and middle-income countries, a protocol for a systematic literature review and narrative synthesis. Syst Rev. 2019;8(1):157. https://doi.org/10.1186/s13643-019-1075-8ArticlePubMedPMC
- 12. Songwathana P, Timalsina R. Disaster preparedness among nurses of developing countries: an integrative review. Int Emerg Nurs. 2021;55:100955. https://doi.org/10.1016/j.ienj.2020.100955ArticlePubMed
- 13. Silavong L, Utriyaprasit K, Wanitkun N, Viwatwongkasem C. A nationwide survey and system analysis of emergency triage system in Lao People’s Democratic Republic. Siriraj Med J. 2023;75(4):241-247. https://doi.org/10.33192/smj.v75i4.260580Article
- 14. Kilpatrick AL, Bouphavanh K, Sengchanh S, Namvongsa V, Gray AZ. Medical education in Lao People’s Democratic Republic: the challenges students face in accessing learning resources. Asia Pac Sch. 2019;4(2):39-47. https://doi.org/10.29060/TAPS.2019-4-2/OA2034Article
- 15. Lao People’s Democratic Republic Ministry of Health. Health sector reform strategy 2021-2030 [Internet]. Lao PDR; 2022 [cited 2025 Jan 18]. Available from: https://rtm.org.la/sector-working-groups/health/
- 16. Suliyong S. Health ministry hosts groundbreaking Continuing Professional Development meeting for nurses and midwives. Vientiane Times [Internet]. 2025 Feb 28 [cited 2025 Feb 28]. Available from: https://www.vientianetimes.org.la/freefreenews/freecontent_042_Health_y25.php
- 17. World Bank. World Development Indicators: current health expenditure (% of GDP) - Lao PDR [Internet]. World Bank; 2024 [cited 2026 Mar 13]. Available from: https://data.worldbank.org/indicator/SH.XPD.CHEX.GD.ZS?locations=LA
- 18. Asian Development Bank (ADB). Enhancing nursing education and training in Asia and the Pacific: ADB Briefs No. 369 [Internet]. ADB; 2025 [cited 2025 Feb 28]. Available from: https://www.adb.org/publications/series/adb-briefs
- 19. Termkitvanich P. Prehospital emergency care. Department of Emergency Medicine, Faculty of Medicine Ramathibodi Hospital, Mahidol University; 2022.
- 20. Thianpratha W, Angkratanirat C, Yuksen C. Emergency care: the pocket guide book. Department of Emergency Medicine, Faculty of Medicine Ramathibodi Hospital, Mahidol University; 2022.
- 21. Yuksen C. Prehospital trauma care. National Institute for Emergency Medicine (NIEM) & Chulabook; 2022.
- 22. United Nations (UN), Department of Economic and Social Affairs. Sustainable Development: the 17 goals [Internet]. UN; 2025 [cited 2025 Jun 19]. Available from: https://sdgs.un.org/goals
- 23. Kang S, Seo H, Ho BD, Nguyen PT. Implementation of a Sustainable Training System for Emergency in Vietnam. Front Public Health. 2018;6:4. https://doi.org/10.3389/fpubh.2018.00004ArticlePubMedPMC
- 24. Kim EM, Ha EH, Kwon MJ. South Korea’s global health outreach through official development assistance: analysis of aid activities of South Korea’s leading aid agencies, 2008-2012. Asia Pac Policy Stud. 2015;2(2):338-346. https://doi.org/10.1002/app5.88Article
- 25. Nam EW. International health cooperation and challenges for official development assistance. Health Policy Manag. 2018;28(3):320-326. https://doi.org/10.4332/KJHPA.2018.28.3.320Article
- 26. Nasr AO. Improving resuscitation practices in low-and middle-income countries: a global imperative. J Acute Care Resusc. 2024;1(3):61-63. https://doi.org/10.4103/jacresus.jacresus_18_24ArticlePubMed
- 27. Thiagarajan S, Semmel DS, Semmel MI. Instructional development for training teachers of exceptional children. Indiana University; 1974. 192 p.
- 28. Purwati Y, Suryani, Asnindari LN. Interprofessional education for maternal and pediatric health curriculum development: focusing on the quality of health education. EAS J Nurs Midwifery [Internet]. 2021 [cited 2025 Jun 19];3(3):126-135. Available from: https://www.easpublisher.com/article/articleID=2146
- 29. National Institute for Emergency Medicine. Pre-hospital trauma care. National Institute for Emergency Medicine; 2021.
- 30. National Institute for Emergency Medicine. Comprehensive emergency care guide book. National Institute for Emergency Medicine; 2021.
- 31. National Institute for Emergency Medicine. Pre-hospital emergency care. National Institute for Emergency Medicine; 2021.
- 32. Doak CC, Doak LG, Root JH. Teaching patients with low literacy skills. 2nd ed. Lippincott; 1996.
- 33. Weintraub D, Maliski SL, Fink A, Choe S, Litwin MS. Suitability of prostate cancer education materials: applying a standardized assessment tool to currently available materials. Patient Educ Couns. 2004;55(2):275-280. https://doi.org/10.1016/j.pec.2003.10.003ArticlePubMed
- 34. Sage O, Wang F, DiAngelo C, Marsden S, Faustini C, Grant S, et al. Enhancing nutrition education resources through the development and refinement of a checklist using the suitability assessment of materials (SAM). Nutr Health. 2026;32(1):31-40. https://doi.org/10.1177/02601060251365357ArticlePubMedPMC
- 35. Sekine M, Goto A, Suzuki T, Onodera M, Kobashi Y, Iseki K. Accessibility of medical information leaflets for patients in emergency care settings in Japan. Health Lit Commun Open. 2025;3(1):2515080. https://doi.org/10.1080/28355245.2025.2515080Article
- 36. Flesch R. A new readability yardstick. J Appl Psychol. 1948;32(3):221-233. https://doi.org/10.1037/h0057532ArticlePubMedPMC
- 37. Richey RC, Klein JD. Design and development research: methods, strategies, and issues. Routledge; 2014. 200. https://doi.org/10.4324/9780203826034Article
- 38. Indaryanti RB, Harsono H, Sutama S, Murtiyasa B, Soemardjoko B. 4D research and development model: trends, challenges, and opportunities review. J Kajian Ilmiah. 2025;25(1):91-98. https://doi.org/10.31599/na7deq07Article
- 39. Aung KT. Nurse empowerment through dynamic xMOOCs using a 4D development model approach. In: Jesus A, editor. Technological approaches to medical and pharmaceutical education. IGI Global Scientific Publishing; 2025. p. 185-222. https://doi.org/10.4018/979-8-3373-1127-2.ch006Article
- 40. Ndung’u A, Ndirangu E, Sarki A, Isiaho L. A cross-sectional study of self-perceived educational needs of emergency nurses in two tertiary hospitals in Nairobi, Kenya. J Emerg Nurs. 2022;48(4):467-476. https://doi.org/10.1016/j.jen.2022.04.001ArticlePubMed
- 41. Dulandas R, Brysiewicz P. A description of the self-perceived educational needs of emergency nurses in Durban, KwaZulu-Natal, South Africa. Afr J Emerg Med. 2018;8(3):84-88. https://doi.org/10.1016/j.afjem.2018.03.001ArticlePubMedPMC
- 42. Suamchaiyaphum K, Jones AR, Fazeli PL. Factors associated with triage clinical decision-making among emergency nurses: a scoping review. J Nurs Care Qual. 2026;41(2):134-141. https://doi.org/10.1097/NCQ.0000000000000903ArticlePubMed
- 43. Said NB, Molassiotis A, Chiang VCL. Psychological first aid training in disaster preparedness for nurses working with emergencies and traumas. Int Nurs Rev. 2022;69(4):548-558. https://doi.org/10.1111/inr.12749ArticlePubMed
- 44. Vongphoumy I, Phongmany P, Sydala S, Prasith N, Reintjes R, Blessmann J. Snakebites in two rural districts in Lao PDR: community-based surveys disclose high incidence of an invisible public health problem. PLoS Negl Trop Dis. 2015;9(6):e0003887. https://doi.org/10.1371/journal.pntd.0003887ArticlePubMedPMC
- 45. Aga AM, Mulugeta D, Motuma A, Wakitole B, Muleta D, Ferede H, et al. Health professionals’ knowledge, attitudes, and practices in snakebite management: a study from high-burden areas in the Afar Region, Ethiopia. PLoS Negl Trop Dis. 2025;19(11):e0013713. https://doi.org/10.1371/journal.pntd.0013713ArticlePubMedPMC
- 46. Robinson SJ, Ritchie AM, Pacilli M, Nestel D, McLeod E, Nataraja RM. Simulation-based education of health workers in low- and middle-income countries: a systematic review. Glob Health Sci Pract. 2024;12(6):e2400187. https://doi.org/10.9745/GHSP-D-24-00187ArticlePubMedPMC
- 47. Mkubwa B, Angwenyi V, Pacione L, Nzioka B, John M, Kibirige N, et al. Contextualization and adaptation of the child and adolescent mental and behavioural disorders module of the mhGAP-IG in Kilifi and Nairobi counties in Kenya. Glob Ment Health (Camb). 2025;12:e92. https://doi.org/10.1017/gmh.2025.10049ArticlePubMedPMC
- 48. Strasser RP, Wright J, Abdalla ME, Van Schaik L, Muller JV. Editorial: Distributed training and rural health professions education. Front Med (Lausanne). 2025;12:1704188. https://doi.org/10.3389/fmed.2025.1704188ArticlePubMedPMC
- 49. Guillaume D, Troncoso E, Duroseau B, Bluestone J, Fullerton J. Mobile-social learning for continuing professional development in low- and middle-income countries: integrative review. JMIR Med Educ. 2022;8(2):e32614. https://doi.org/10.2196/32614ArticlePubMedPMC
References
Appendix
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
 ePub Link
ePub Link Cite
CiteDevelopment of emergency nursing educational materials in Lao People's Democratic Republic: a methodological study
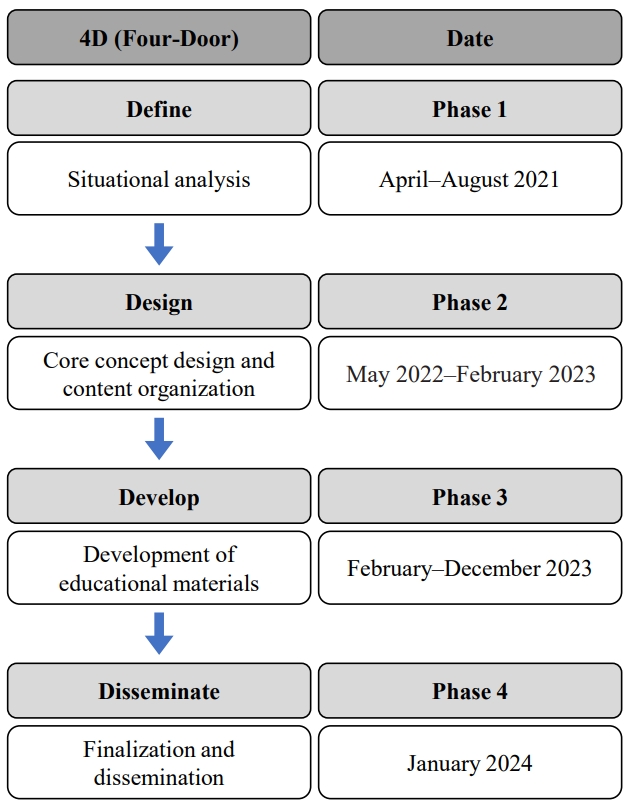
Fig. 1. Research process based on the 4D (Four-Door) Model.
Fig. 1.
Development of emergency nursing educational materials in Lao People's Democratic Republic: a methodological study
| Key finding | Description |
|---|---|
| Deficiency in professional emergency nursing competencies | Significant lack of skills in immediate response capabilities during emergencies |
| Inadequate proficiency in emergency equipment utilization | Despite the availability of modern equipment (AEDs, monitoring devices), proper utilization remains problematic |
| Absence of standardized emergency protocols | Lack of established protocols and educational materials creates inconsistency in mental health care quality across institutions |
| Restricted educational opportunities | Limited access to training due to bureaucratic requirements and insufficient availability of international-standard programs |
| Need for specialized preparation for unique circumstances in Lao PDR | Requirement for training specifically addressing traffic accidents, infectious diseases, and maternal emergencies |
| Category | Mean±SD |
|---|---|
| Knowledge | |
| Basic life support | 4.78±0.45 |
| Advanced cardiac life support | 4.76±0.47 |
| Post-resuscitation care | 4.75±0.51 |
| Skill | |
| Intubation management | 4.75±0.47 |
| Ventilator management | 4.74±0.52 |
| Isolation technology | 4.66±0.54 |
| Domain | Content | Level | Contribution |
|---|---|---|---|
| 1. Introduction | - | Collaborative university | |
| 2. Primary assessment of ER patients | 2.1 Food poisoning | Low | A Hospital |
| 2.2 Gastrointestinal bleeding | |||
| 3. Triage | 3.1 Guidelines for triage of emergency patients | Low | B Hospital |
| 4. Basic life support | 4.1 Cardiopulmonary resuscitation basic life support | Low | C Hospital |
| 4.2 Advanced life support | |||
| 4.3 Cardiopulmonary resuscitation in children | |||
| 5. Respiratory emergency interventions | 5.1 Airway obstruction | High | B Hospital |
| 6. Nursing care plan of trauma and non-trauma patients | 6.1 Hypoglycemic shock patients | High | A Hospital |
| 6.2 Hypotension patients due to blood loss | |||
| 6.3 Cardiogenic shock patients | |||
| 6.4 Ischemic and hemorrhagic stroke in shock patients | |||
| 6.5 Abdominal trauma | |||
| 6.6 Broken arm & leg | |||
| 6.7 Head trauma | |||
| 6.8 Neck trauma | |||
| 6.9 Spinal trauma | |||
| 7. Application of pharmacology for ER | 7.1 Respiratory-asthma | Medium | C Hospital |
| 7.2 Respiratory-airway obstruction | |||
| 7.3 Respiratory-anaphylactic shock | |||
| 7.4 Food poisoning | |||
| 8. Nursing management of snakebite patients | 8.1 Snakebite patients | Medium | C Hospital |
| Domain | Content |
|---|---|
| 1. Introduction | 1.1 Emergency nursing competencies in Lao PDR |
| 1.2 Scope and standards of emergency nursing in Lao PDR | |
| 1.3 Emergency nursing ethics and regulations | |
| 2. Primary assessment of ER patients | 2.1 Vital sign assessment (BT, BP, PR, RR, SpO2), Glasgow Coma Scale (GCS), Basic Head to Toe assessment |
| 3. Triage | 3.1 Guidelines for triage of emergency patients |
| 3.2 Pain control | |
| 4. Basic life support | 4.1 Cardiopulmonary resuscitation basic life support |
| 4.2 Advanced life support | |
| 4.3 Cardiopulmonary resuscitation in children | |
| 5. Respiratory emergency interventions | 5.1 Emergency nursing care of a patient with airway obstruction |
| 5.2 Emergency nursing care of a patient with pneumonia | |
| 5.3 Emergency nursing care of a patient with chest injury | |
| 5.4 Emergency nursing care of a patient with frontal osteomyelitis | |
| 6. Nursing care of trauma patients | 6.1 Emergency nursing care of a patient with abdominal trauma |
| 6.2 Emergency nursing care of a patient with broken arm | |
| 6.3 Emergency nursing care of a patient with broken leg | |
| 6.4 Emergency nursing care of a patient with head trauma | |
| 6.5 Emergency nursing care of a patient with c-spine trauma | |
| 6.6 Emergency nursing care of a patient with spinal trauma | |
| 7. Nursing care of non-trauma patients | 7.1 Emergency nursing care of hypovolemic shock patients |
| 7.2 Emergency nursing care for cardiogenic shock patients | |
| 7.3 Emergency nursing care for ischemic stroke in shock patients | |
| 7.4 Emergency nursing care for hemorrhagic stroke in shock patients | |
| 8. Nursing interventions for ER patients | 8.1 Nursing interventions for food poisoning |
| 8.2 Nursing interventions for gastrointestinal bleeding | |
| 8.3 Nursing interventions for hypoglycemia | |
| 8.4 Nursing interventions for hyperglycemia | |
| 8.5 Nursing interventions for asthma | |
| 8.6 Nursing interventions for anaphylactic shock | |
| 9. Nursing management of snakebite patients | 9.1 Nursing care of snakebite patients |
| 10. Psychological emergency interventions | 10.1 Psychological emergency interventions |
Table 1. Current status and problems of emergency nursing in hospitals in Lao PDR
AED, automated external defibrillator; Lao PDR, Lao People’s Democratic Republic.
Table 2. Priority knowledge and skill domains in emergency nursing (N=70)
SD, standard deviation.
Table 3. Initial framework of emergency nursing educational domains
ER, emergency room.
Table 4. Final domains and contents of emergency nursing education materials
ER, emergency room; Lao PDR, Lao People’s Democratic Republic; BT, body temperature; BP, blood pressure; PR, pulse rate; RR, respiration rate; SpO2, oxygen saturation; GCS, Glasgow Coma Scale.

