 Submit an article
Submit an article
Articles
- Page Path
- HOME > J Korean Acad Nurs > Ahead-of print articles > Article
-
Research Paper
국립 특수 병원 간호사의 간호관리역량: 혼합연구방법 -
최지영1,*
 , 황지인1,2
, 황지인1,2 - Nursing management competencies among nurses in national specialized hospitals in Korea: a mixed-methods study
-
Jiyoung Choi1,*, Jee-In Hwang1,2
-
DOI: https://doi.org/10.4040/jkan.25175
Published online: May 22, 2026
1경희대학교 공공대학원 의료관리학과
2경희대학교 간호과학대학
1Department of Healthcare Management, Graduate School of Public Policy & Civic Engagement Kyung Hee University, Seoul, South Korea
2College of Nursing Science, Kyung Hee University, Seoul, South Korea
- Corresponding author: Jee-In Hwang College of Nursing Science, Kyung Hee University, 26 Kyungheedae-ro, Dongdaemoon-gu, Seoul 02447, South Korea E-mail: jihwang@khu.ac.kr
-
*Current affiliation: Department of Nursing, Graduate School, Kyung Hee University, Seoul, South Korea.
†This manuscript is a revision of the first author’s master’s thesis from Kyung Hee University in 2025.
• Received: December 13, 2025 • Revised: February 1, 2026 • Accepted: February 26, 2026
© 2026 Korean Society of Nursing Science
This is an Open Access article distributed under the terms of the Creative Commons Attribution NoDerivs License (http://creativecommons.org/licenses/by-nd/4.0) If the original work is properly cited and retained without any modification or reproduction, it can be used and re-distributed in any format and medium.
- 94 Views
- 9 Download
Abstract
-
Purpose
- This study aimed to examine nursing management competencies among nurses working in national specialized hospitals, to identify competency development needs and influencing factors, and to provide foundational data for the development of educational and competency-enhancement programs.
-
Methods
- A mixed-methods design was employed. Quantitative data were collected via an online survey of 162 nurses from five national specialized hospitals from January 10 to February 10, 2025, and qualitative data were obtained through in-depth interviews with 20 participants from March 7 to April 16, 2025. Quantitative data were analyzed using descriptive statistics, independent t-tests, analysis of variance, importance–performance analysis, the Borich Needs Assessment, the Locus for Focus model, and multiple regression analysis. Qualitative data were analyzed using content analysis with ATLAS.ti.
-
Results
- The mean performance score for nursing management competencies was 3.56±0.71 on a 5-point scale. Customer orientation received the highest score (4.03±0.78), whereas business and marketing received the lowest score (2.92±1.03). Across needs-assessment models, leadership, nursing ethics and law, quality improvement, and standard development consistently emerged as high-priority areas. In multiple regression analysis, the nursing work environment was the only factor significantly associated with nursing management competency performance (β=.33, p<.001). Qualitative content analysis corroborated these findings and identified three facilitator themes and three barrier themes.
-
Conclusion
- Nursing management competency performance among nurses in national specialized hospitals was associated with the nursing work environment, including organizational conditions. These findings underscore the importance of organizational support and suggest that competency-based education should be redesigned to prioritize high-need competency areas. This study provides a foundation for developing educational interventions and programs to enhance nursing management capacity.
서론
방법
1) 일반적 특성
2) 간호관리역량
3) 간호근무환경
결과
1) 대상자의 일반적 특성
2) 간호관리역량 수행도 수준과 간호근무환경
3) 간호관리역량 중요도와 요구도 분석
4) 간호관리역량 수행도에 영향을 미치는 요인
1) 간호관리역량의 촉진요인
(1) 주제1: 학습과 조직적 지원을 통한 간호관리역량 개발의 기반 형성
(2) 주제2: 현장 중심의 주도성과 실무경험의 통합을 통한 간호관리역량 발휘
(3) 주제3: 상호작용과 협력을 통한 간호관리 실천
2) 간호관리역량의 방해요인
(1) 주제1: 개인의 수동성과 변화 저항으로 인한 한계
(2) 주제2: 비효율적 조직구조와 제도적 한계
(3) 주제3: 자원ㆍ협업ㆍ교육체계의 부족으로 인한 간호관리 실행의 제약
고찰
결론
-
Conflicts of Interest
No potential conflict of interest relevant to this article was reported.
-
Acknowledgements
None.
-
Funding
This research received no external funding.
-
Data Sharing Statement
Please contact the corresponding author for data availability.
-
Author Contributions
Conceptualization or/and Methodology: JYC, JIH. Data curation or/and Analysis: JYC. Funding acquisition: none. Investigation: JYC. Project administration or/and Supervision: JIH. Resources or/and Software: JYC. Validation: JYC, JIH. Visualization: JYC. Writing: original draft or/and Review & Editing: JYC, JIH. Final approval of the manuscript: all authors.
Article Information
Fig. 1.Importance–performance analysis and the locus for focus model of nursing managerial competencies. (A) Importance–performance analysis of nursing managerial competencies. (B) The locus for focus model of nursing managerial competencies.
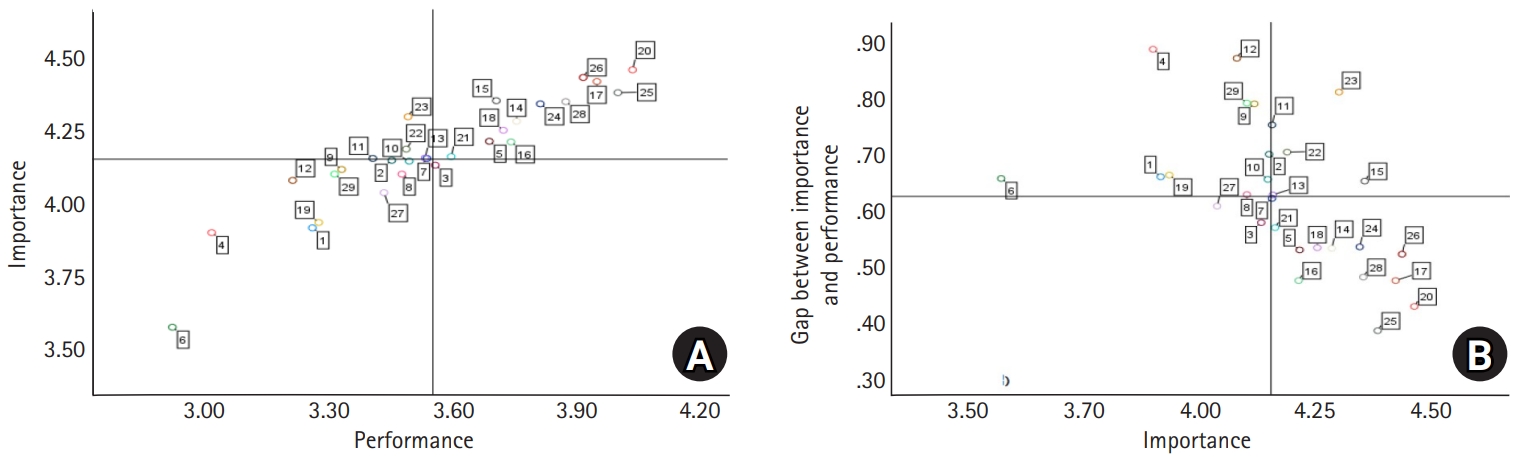
Table 1.Differences in nursing management competency performance according to general characteristics (N=162)
| Characteristic | n (%) | Mean±SD | Performance | |
|---|---|---|---|---|
| Mean±SD | t or F (p)a) | |||
| Gender | .68 (.496) | |||
| Women | 130 (80.2) | 3.58±0.72 | ||
| Men | 32 (19.8) | 3.49±0.68 | ||
| Age (yr) | 39.56±8.14 | 10.07 (<.001)1<3 | ||
| ≤39 | 89 (55.0) | 3.38±0.68 | ||
| 40–49 | 47 (29.0) | 3.67±0.63 | ||
| ≥50 | 26 (16.0) | 4.02±0.69 | ||
| Education level | 14.03 (<.001)1,2<3 | |||
| Diploma | 13 (8.0) | 3.11±0.51 | ||
| Bachelor’s | 104 (64.2) | 3.44±0.70 | ||
| ≥Master’s | 45 (27.8) | 3.98±0.59 | ||
| Marital status | –3.51 (<.001) | |||
| Unmarried | 58 (35.8) | 3.31±0.74 | ||
| Married | 104 (64.2) | 3.71±0.65 | ||
| Clinical experience (yr) | 15.73±8.09 | 9.02 (<.001)1<4 | ||
| <15 | 86 (53.1) | 3.35±0.70 | ||
| 15–<20 | 38 (23.5) | 3.65±0.60 | ||
| 20–<25 | 15 (9.3) | 3.73±0.67 | ||
| ≥25 | 23 (14.1) | 4.12±0.58 | ||
| Current hospital career (yr) | 8.51±8.30 | 10.64b) (<.001)1<3,4 | ||
| <10 | 116 (71.6) | 3.40±0.65 | ||
| 10–<15 | 15 (9.3) | 3.92±0.88 | ||
| 15–<20 | 10 (6.2) | 3.79±0.37 | ||
| ≥20 | 21 (13.0) | 4.14±0.59 | ||
| Work department | 3.80 (.024)1<3 | |||
| Ward | 109 (67.3) | 3.46±0.72 | ||
| Outpatient clinic | 16 (9.9) | 3.71±0.56 | ||
| Others | 37 (22.8) | 3.81±0.66 | ||
| Work schedule | –5.20 (<.001) | |||
| Shift work | 95 (58.6) | 3.34±0.67 | ||
| Non-shift work | 67 (41.4) | 3.88±0.64 | ||
| Position | 10.96 (<.001)1<2,3 | |||
| Staff nurse | 126 (77.8) | 3.43±0.68 | ||
| Charge nurse | 10 (6.2) | 4.02±0.69 | ||
| ≥Head nurse | 26 (16.0) | 4.02±0.56 | ||
| Research experience | 3.71 (<.001) | |||
| Yes | 57 (35.2) | 3.83±0.61 | ||
| No | 105 (64.8) | 3.42±0.71 | ||
| Education on nursing management competency | 3.99 (<.001) | |||
| Yes | 90 (55.6) | 3.75±0.66 | ||
| No | 72 (44.4) | 3.33±0.69 | ||
Table 2.Analysis of importance, performance, and needs of nursing management competencies (N=162)
| Variable | No. of items | Mean±SD | Paired t | IPA (quadrant) | Borich needs | LF | Priority competency | ||
|---|---|---|---|---|---|---|---|---|---|
| Importance | Performance | Score | Rank | ||||||
| Planning process | |||||||||
| 1. Vision building | 2 | 3.91±0.76 | 3.26±0.97 | 12.16* | III | 2.57 | (13) | LH | |
| 2. Planning | 3 | 4.15±0.70 | 3.45±0.81 | 11.62* | III | 2.89 | (8) | LH | |
| 3. Analysis | 4 | 4.13±0.65 | 3.55±0.83 | 10.30* | IV | 2.38 | (17) | LL | |
| 4. Budget & fiscal management | 3 | 3.90±0.86 | 3.01±1.03 | 11.30* | III | 3.45 | (3) | LH | |
| 5. Decision-making | 3 | 4.21±0.77 | 3.69±0.82 | 10.24* | I | 2.22 | (24) | HL | |
| 6. Business & marketing | 2 | 3.57±1.00 | 2.92±1.03 | 9.96* | III | 2.34 | (19) | LH | |
| Sub-total | 4.01±0.65 | 3.35±0.75 | |||||||
| Organizing process | |||||||||
| 7. Organization management | 4 | 4.15±0.70 | 3.53±0.84 | 10.73* | II | 2.57 | (14) | HL | |
| 8. Innovation & change management | 3 | 4.10±0.69 | 3.47±0.87 | 11.22* | III | 2.56 | (15) | LH | |
| Sub-total | 4.13±0.65 | 3.51±0.80 | |||||||
| Human resources management process | |||||||||
| 9. Staffing management | 5 | 4.11±0.70 | 3.33±0.95 | 11.75* | III | 3.24 | (4) | LH | |
| 10. Human resources development & staff education | 7 | 4.14±0.66 | 3.49±0.83 | 12.30* | III | 2.70 | (10) | LH | |
| Sub-total | 4.13±0.63 | 3.42±0.82 | |||||||
| Directing process | |||||||||
| 11. Leadership | 4 | 4.15±0.76 | 3.40±0.96 | 10.86* | II | 3.11 | (6) | HH | a) |
| 12. Professionalism | 4 | 4.08±0.73 | 3.21±0.95 | 12.54* | III | 3.54 | (1) | LH | |
| 13. Nursing ethics & law | 4 | 4.15±0.72 | 3.53±0.88 | 11.11* | II | 2.60 | (12) | HH | a) |
| 14. Communication & interpersonal relationships | 7 | 4.28±0.69 | 3.75±0.79 | 10.47* | I | 2.27 | (22) | HL | |
| 15. Cooperation & mediation | 4 | 4.35±0.70 | 3.70±0.89 | 10.81* | I | 2.83 | (9) | HH | |
| 16. Motivation | 2 | 4.21±0.75 | 3.74±0.91 | 8.92* | I | 1.99 | (27) | HL | |
| 17. Problem-solving | 4 | 4.42±0.64 | 3.95±0.74 | 9.50* | I | 2.09 | (25) | HL | |
| 18. Conflict management | 2 | 4.25±0.74 | 3.72±0.88 | 9.20* | I | 2.26 | (23) | HL | |
| 19. Negotiation | 2 | 3.93±0.93 | 3.27±1.13 | 10.98* | III | 2.60 | (11) | LH | |
| 20. Customer orientation | 4 | 4.46±0.68 | 4.03±0.78 | 10.06* | I | 1.90 | (28) | HL | |
| 21. Self-management | 5 | 4.16±0.66 | 3.59±0.80 | 10.41* | I | 2.36 | (18) | HL | |
| Sub-total | 4.24±0.61 | 3.64±0.74 | |||||||
| Control process | |||||||||
| 22. Quality improvement | 3 | 4.19±0.82 | 3.48±0.96 | 10.48* | II | 2.94 | (7) | HH | a) |
| 23. Development of nursing standard | 3 | 4.30±0.73 | 3.49±0.99 | 11.13* | II | 3.47 | (2) | HH | a) |
| 24. Nursing practice | 7 | 4.34±0.67 | 3.81±0.85 | 10.00* | I | 2.31 | (20) | HL | |
| 25. Resource management | 2 | 4.38±0.68 | 4.00±0.85 | 7.27* | I | 1.68 | (29) | HL | |
| 26. Patient safety & infection management | 6 | 4.43±0.61 | 3.91±0.82 | 10.72* | I | 2.30 | (21) | HL | |
| 27. Information management | 6 | 4.03±0.71 | 3.43±0.86 | 12.35* | III | 2.44 | (16) | LL | |
| 28. Accreditation preparation | 2 | 4.35±0.78 | 3.87±0.92 | 6.85* | I | 2.08 | (26) | HL | |
| 29. Performance management | 6 | 4.10±0.76 | 3.31±1.10 | 11.25* | III | 3.23 | (5) | LH | |
| Sub-total | 4.25±0.59 | 3.63±0.76 | |||||||
| Total | 113 | 4.19±0.57 | 3.56±0.71 | ||||||
Quadrant I: high importance/high performance; Quadrant II: high importance/low performance; Quadrant III: low importance/low performance; Quadrant IV: low importance/high performance.
HH, high discrepancy/high importance; HL, high discrepancy/low importance; IPA, importance performance analysis; LF, locus for focus; LH, low discrepancy/high importance; LL, low discrepancy/low importance; SD, standard deviation.
*p<.001.
a)Priority competency items.
Table 3.Factors influencing the performance of nursing management competencies (N=162)
Table 4.Facilitators and barriers of nursing management competency
- 1. Lee SH, Choi KS, Kang HY, Cho WH, Chae YM. Factors associated with the degree of quality improvement implementation. Korean J Prev Med. 2001;34(4):363-371.
- 2. Oh YH. Problem with and policy agenda for public health services in Korea. Health Welf Policy Forum. 2013;(200):62-82. https://doi.org/10.23062/2013.06.7Article
- 3. Institute of Medicine (US) Committee on the Robert Wood Johnson Foundation Initiative on the Future of Nursing, at the Institute of Medicine. The future of nursing: leading change, advancing health. National Academies Press (US); 2011. 671. https://doi.org/10.17226/12956
- 4. Song YO, Kim H, Nam Y, Choe K, Ha J. Effects of a competency-based education program for inpatient psychiatric nurses: a pre-post intervention study. J Korean Acad Psychiatr Ment Health Nurs. 2022;31(1):80-87. https://doi.org/10.12934/jkpmhn.2022.31.1.80Article
- 5. Lee T, Kim I, Kim E, Jung J, Kang K. Educational need of nursing managerial competency in the hospitals. J Korean Acad Nurs Adm [Internet]. 2006 [cited 2025 Dec 5];12(1):113-121. Available from: https://www.koreascience.kr/article/JAKO200628835720115.pub?&lang=ko
- 6. Choi SH, Lee SY, Jo D, Jung Y. ROK military nurse managers’ perception on the importance and performance of clinical nursing managerial competencies. Korean J Mil Nurs Res. 2020;38(1):38-54. https://doi.org/10.31148/kjmnr.2020.38.1.38Article
- 7. Yu BH, Jang KS. Priority need analysis for career level-based nursing management competency development of advanced general hospital nurses. J Korean Acad Nurs Adm. 2022;28(4):417-429. https://doi.org/10.11111/jkana.2022.28.4.417Article
- 8. Kang G, Kim JH. Clinical nurses’ perception on the importance and performance of nursing managerial competencies. J Korean Acad Soc Nurs Educ. 2017;23(3):252-267. https://doi.org/10.5977/jkasne.2017.23.3.252Article
- 9. Abdul-Rahim HZ, Sharbini SH, Ali M, Hashim SH, Abdul-Mumin KH. Leadership and management skills for student nurses: a scoping review. BMC Nurs. 2025;24(1):111. https://doi.org/10.1186/s12912-024-02603-7ArticlePubMedPMC
- 10. Lee TH, Kang KH, Lee SH, Ko YK, Park JS, Lee SR, et al. Development of the core task and competency matrix for unit managers. J Korean Clin Nurs Res. 2017;23(2):189-201. https://doi.org/10.22650/JKCNR.2017.23.2.189Article
- 11. Kim S, Jeong JH, Shin HK, Choi SJ. Development of management competency enhancement program for middle-level nursing managers. J Korean Clin Nurs Res. 2023;29(1):107-120. https://doi.org/10.22650/JKCNR.2023.29.1.107Article
- 12. Byeon HS, Jang KS. A study on the nursing managerial competency of head nurses in general hospitals. Chonnam J Nurs Sci [Internet]. 2000 [cited 2025 Dec 5];5(1):135-150. Available from: https://crins530.jnuac.kr/bbs/board.php?bo_table=journal2&wr_id=57&page=9
- 13. Westerman JW, Simmons BL. The effects of work environment on the personality-performance relationship: an exploratory study. J Manag Issues. 2007;19(2):288-305.
- 14. Lee R, Kim M, Choi S, Shin HY. Factors influencing managerial competence of frontline nurse managers. J Korean Acad Nurs Adm. 2018;24(5):435-444. https://doi.org/10.11111/jkana.2018.24.5.435Article
- 15. Park JM, Shin NY. Nursing work environment and job stress of nurses: effects on job performance of nurses in the intensive care unit. J Korean Soc Multicult Health. 2023;13(1):75-83. https://doi.org/10.33502/JKSMH.13.1.075Article
- 16. Kutney-Lee A, Stimpfel AW, Sloane DM, Cimiotti JP, Quinn LW, Aiken LH. Changes in patient and nurse outcomes associated with magnet hospital recognition. Med Care. 2015;53(6):550-557. https://doi.org/10.1097/MLR.0000000000000355ArticlePubMedPMC
- 17. Kang Y, Kim JH. Influence of emotional intelligence of experienced nurses on nursing managerial competence: focusing on the mediating effect of communication competence. J Korean Acad Nurs Adm. 2024;30(1):79-90. https://doi.org/10.11111/jkana.2024.30.1.79Article
- 18. Creswell JW. Research design: qualitative, quantitative, and mixed methods approaches. 4th ed. Sage Publications; 2014. 342 p.
- 19. Kim SY, Kim JK. A study on the classification of nursing management competencies and development of related behavioral indicators in hospitals. J Korean Acad Nurs. 2016;46(3):375-389. https://doi.org/10.4040/jkan.2016.46.3.375ArticlePubMed
- 20. Lynn MR. Determination and quantification of content validity. Nurs Res. 1986;35(6):382-385. https://doi.org/10.1097/00006199-198611000-00017ArticlePubMed
- 21. Polit DF, Beck CT, Owen SV. Is the CVI an acceptable indicator of content validity?: appraisal and recommendations. Res Nurs Health. 2007;30(4):459-467. https://doi.org/10.1002/nur.20199ArticlePubMed
- 22. Lake ET. Development of the Practice Environment Scale of the Nursing Work Index. Res Nurs Health. 2002;25(3):176-188. https://doi.org/10.1002/nur.10032ArticlePubMed
- 23. Cho E, Choi M, Kim EY, Yoo IY, Lee NJ. Construct validity and reliability of the Korean version of the practice environment scale of nursing work index for Korean nurses. J Korean Acad Nurs. 2011;41(3):325-332. https://doi.org/10.4040/jkan.2011.41.3.325ArticlePubMed
- 24. Lee JA. Managerial competencies of nurse unit manager: a mixed method study [dissertation]. Seoul: Ewha Womans University; 2021.
- 25. Martens J, Motz J, Stump L. A certified registered nurse anesthetist’s transition to manager. AANA J. 2018;86(6):447-454. PubMed
- 26. Martilla JA, James JC. Importance-performance analysis. J MarK. 1977;41(1):77-79. https://doi.org/10.1177/002224297704100112Article
- 27. Borich GD. A needs assessment model for conducting follow-up studies. J Teach Educ. 1980;31(3):39-42. https://doi.org/10.1177/002248718003100310Article
- 28. Mink OG, Shultz JM, Mink BP. Developing and managing open organizations: a model and methods for maximizing organizational potential. 2nd ed. Somerset Consulting Group; 1991. 284 p.
- 29. Jeong HK, Moon S. Need analysis for managerial competencies of nurse managers in general hospitals. J Korean Acad Soc Nurs Educ. 2024;30(1):82-95. https://doi.org/10.5977/jkasne.2024.30.1.82Article
- 30. Hsieh HF, Shannon SE. Three approaches to qualitative content analysis. Qual Health Res. 2005;15(9):1277-1288. https://doi.org/10.1177/1049732305276687ArticlePubMed
- 31. Lincoln YS, Guba EG. Naturalistic inquiry. Sage Publications; 1985. 416 p.
- 32. Hong MH, Park JY. Nurses’ perception of accreditation, awareness and performance of infection control in an accredited healthcare system. J Korean Acad Nurs Adm. 2016;22(2):167-177. https://doi.org/10.11111/jkana.2016.22.2.167Article
- 33. Kwon MJ, Yi Y. Factors influencing on performance for infection control of nurses working in comprehensive nursing care service ward under COVID-19 pandemic. J Korean Acad Nurs Adm. 2022;28(2):121-130. https://doi.org/10.11111/jkana.2022.28.2.121Article
- 34. Kim BM, Lee YM, Yoon SH, Choi EO. A study of the head nurse’s leadership and the organizational effectiveness as perceived by staff nurses. J Korean Acad Nurs Adm. 2007;13(3):373-383.
- 35. Yom YH, Noh SM, Kim KH. Clinical nurses’ experience of positive organizational culture. J Korean Acad Nurs Adm. 2014;20(5):469-480. http://doi.org/10.11111/jkana.2014.20.5.469Article
References
Appendix
Appendix 1.
The original version of nursing management competencies was derived from Kang and Kim [8] (2017).
Appendix 2.
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
 ePub Link
ePub Link Cite
CiteNursing management competencies among nurses in national specialized hospitals in Korea: a mixed-methods study
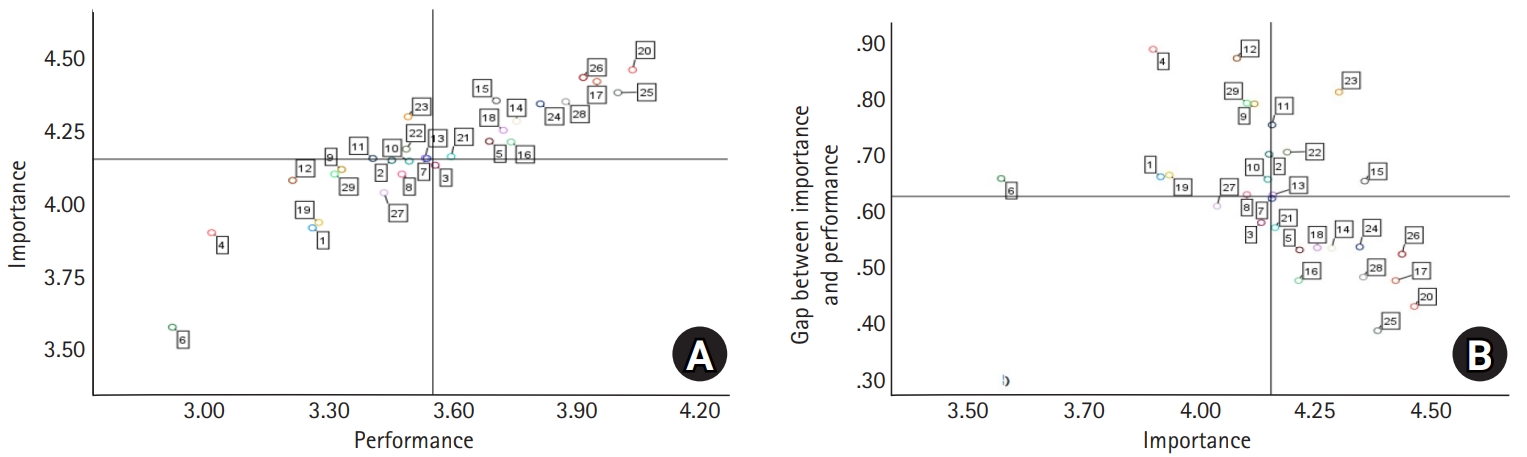
Fig. 1. Importance–performance analysis and the locus for focus model of nursing managerial competencies. (A) Importance–performance analysis of nursing managerial competencies. (B) The locus for focus model of nursing managerial competencies.
Fig. 1.
Nursing management competencies among nurses in national specialized hospitals in Korea: a mixed-methods study
| Characteristic | n (%) | Mean±SD | Performance | |
|---|---|---|---|---|
| Mean±SD | t or F (p) |
|||
| Gender | .68 (.496) | |||
| Women | 130 (80.2) | 3.58±0.72 | ||
| Men | 32 (19.8) | 3.49±0.68 | ||
| Age (yr) | 39.56±8.14 | 10.07 (<.001)1<3 | ||
| ≤39 | 89 (55.0) | 3.38±0.68 | ||
| 40–49 | 47 (29.0) | 3.67±0.63 | ||
| ≥50 | 26 (16.0) | 4.02±0.69 | ||
| Education level | 14.03 (<.001)1,2<3 | |||
| Diploma | 13 (8.0) | 3.11±0.51 | ||
| Bachelor’s | 104 (64.2) | 3.44±0.70 | ||
| ≥Master’s | 45 (27.8) | 3.98±0.59 | ||
| Marital status | –3.51 (<.001) | |||
| Unmarried | 58 (35.8) | 3.31±0.74 | ||
| Married | 104 (64.2) | 3.71±0.65 | ||
| Clinical experience (yr) | 15.73±8.09 | 9.02 (<.001)1<4 | ||
| <15 | 86 (53.1) | 3.35±0.70 | ||
| 15–<20 | 38 (23.5) | 3.65±0.60 | ||
| 20–<25 | 15 (9.3) | 3.73±0.67 | ||
| ≥25 | 23 (14.1) | 4.12±0.58 | ||
| Current hospital career (yr) | 8.51±8.30 | 10.64 |
||
| <10 | 116 (71.6) | 3.40±0.65 | ||
| 10–<15 | 15 (9.3) | 3.92±0.88 | ||
| 15–<20 | 10 (6.2) | 3.79±0.37 | ||
| ≥20 | 21 (13.0) | 4.14±0.59 | ||
| Work department | 3.80 (.024)1<3 | |||
| Ward | 109 (67.3) | 3.46±0.72 | ||
| Outpatient clinic | 16 (9.9) | 3.71±0.56 | ||
| Others | 37 (22.8) | 3.81±0.66 | ||
| Work schedule | –5.20 (<.001) | |||
| Shift work | 95 (58.6) | 3.34±0.67 | ||
| Non-shift work | 67 (41.4) | 3.88±0.64 | ||
| Position | 10.96 (<.001)1<2,3 | |||
| Staff nurse | 126 (77.8) | 3.43±0.68 | ||
| Charge nurse | 10 (6.2) | 4.02±0.69 | ||
| ≥Head nurse | 26 (16.0) | 4.02±0.56 | ||
| Research experience | 3.71 (<.001) | |||
| Yes | 57 (35.2) | 3.83±0.61 | ||
| No | 105 (64.8) | 3.42±0.71 | ||
| Education on nursing management competency | 3.99 (<.001) | |||
| Yes | 90 (55.6) | 3.75±0.66 | ||
| No | 72 (44.4) | 3.33±0.69 | ||
| Variable | No. of items | Mean±SD | Paired t | IPA (quadrant) | Borich needs | LF | Priority competency | ||
|---|---|---|---|---|---|---|---|---|---|
| Importance | Performance | Score | Rank | ||||||
| Planning process | |||||||||
| 1. Vision building | 2 | 3.91±0.76 | 3.26±0.97 | 12.16 |
III | 2.57 | (13) | LH | |
| 2. Planning | 3 | 4.15±0.70 | 3.45±0.81 | 11.62 |
III | 2.89 | (8) | LH | |
| 3. Analysis | 4 | 4.13±0.65 | 3.55±0.83 | 10.30 |
IV | 2.38 | (17) | LL | |
| 4. Budget & fiscal management | 3 | 3.90±0.86 | 3.01±1.03 | 11.30 |
III | 3.45 | (3) | LH | |
| 5. Decision-making | 3 | 4.21±0.77 | 3.69±0.82 | 10.24 |
I | 2.22 | (24) | HL | |
| 6. Business & marketing | 2 | 3.57±1.00 | 2.92±1.03 | 9.96 |
III | 2.34 | (19) | LH | |
| Sub-total | 4.01±0.65 | 3.35±0.75 | |||||||
| Organizing process | |||||||||
| 7. Organization management | 4 | 4.15±0.70 | 3.53±0.84 | 10.73 |
II | 2.57 | (14) | HL | |
| 8. Innovation & change management | 3 | 4.10±0.69 | 3.47±0.87 | 11.22 |
III | 2.56 | (15) | LH | |
| Sub-total | 4.13±0.65 | 3.51±0.80 | |||||||
| Human resources management process | |||||||||
| 9. Staffing management | 5 | 4.11±0.70 | 3.33±0.95 | 11.75 |
III | 3.24 | (4) | LH | |
| 10. Human resources development & staff education | 7 | 4.14±0.66 | 3.49±0.83 | 12.30 |
III | 2.70 | (10) | LH | |
| Sub-total | 4.13±0.63 | 3.42±0.82 | |||||||
| Directing process | |||||||||
| 11. Leadership | 4 | 4.15±0.76 | 3.40±0.96 | 10.86 |
II | 3.11 | (6) | HH | |
| 12. Professionalism | 4 | 4.08±0.73 | 3.21±0.95 | 12.54 |
III | 3.54 | (1) | LH | |
| 13. Nursing ethics & law | 4 | 4.15±0.72 | 3.53±0.88 | 11.11 |
II | 2.60 | (12) | HH | |
| 14. Communication & interpersonal relationships | 7 | 4.28±0.69 | 3.75±0.79 | 10.47 |
I | 2.27 | (22) | HL | |
| 15. Cooperation & mediation | 4 | 4.35±0.70 | 3.70±0.89 | 10.81 |
I | 2.83 | (9) | HH | |
| 16. Motivation | 2 | 4.21±0.75 | 3.74±0.91 | 8.92 |
I | 1.99 | (27) | HL | |
| 17. Problem-solving | 4 | 4.42±0.64 | 3.95±0.74 | 9.50 |
I | 2.09 | (25) | HL | |
| 18. Conflict management | 2 | 4.25±0.74 | 3.72±0.88 | 9.20 |
I | 2.26 | (23) | HL | |
| 19. Negotiation | 2 | 3.93±0.93 | 3.27±1.13 | 10.98 |
III | 2.60 | (11) | LH | |
| 20. Customer orientation | 4 | 4.46±0.68 | 4.03±0.78 | 10.06 |
I | 1.90 | (28) | HL | |
| 21. Self-management | 5 | 4.16±0.66 | 3.59±0.80 | 10.41 |
I | 2.36 | (18) | HL | |
| Sub-total | 4.24±0.61 | 3.64±0.74 | |||||||
| Control process | |||||||||
| 22. Quality improvement | 3 | 4.19±0.82 | 3.48±0.96 | 10.48 |
II | 2.94 | (7) | HH | |
| 23. Development of nursing standard | 3 | 4.30±0.73 | 3.49±0.99 | 11.13 |
II | 3.47 | (2) | HH | |
| 24. Nursing practice | 7 | 4.34±0.67 | 3.81±0.85 | 10.00 |
I | 2.31 | (20) | HL | |
| 25. Resource management | 2 | 4.38±0.68 | 4.00±0.85 | 7.27 |
I | 1.68 | (29) | HL | |
| 26. Patient safety & infection management | 6 | 4.43±0.61 | 3.91±0.82 | 10.72 |
I | 2.30 | (21) | HL | |
| 27. Information management | 6 | 4.03±0.71 | 3.43±0.86 | 12.35 |
III | 2.44 | (16) | LL | |
| 28. Accreditation preparation | 2 | 4.35±0.78 | 3.87±0.92 | 6.85 |
I | 2.08 | (26) | HL | |
| 29. Performance management | 6 | 4.10±0.76 | 3.31±1.10 | 11.25 |
III | 3.23 | (5) | LH | |
| Sub-total | 4.25±0.59 | 3.63±0.76 | |||||||
| Total | 113 | 4.19±0.57 | 3.56±0.71 | ||||||
| Variable | Category | B | SE | ß | t | p |
|---|---|---|---|---|---|---|
| Education level | ≥Master’s (ref: bachelor’s & diploma) | 0.18 | 0.15 | .12 | 1.19 | .236 |
| Marital status | Married (ref: unmarried) | 0.15 | 0.11 | .10 | 1.33 | .184 |
| Clinical experience (yr) | 0.00 | 0.01 | .03 | 0.29 | .772 | |
| Work department | Outpatient clinic & others (ref: ward) | –0.29 | 0.19 | –.20 | –1.56 | .120 |
| Work schedule | Non-shift work (ref: shift work) | 0.43 | 0.23 | .30 | 1.89 | .060 |
| Position | ≥Charge nurse (ref: staff nurse) | –0.13 | 0.18 | –.08 | –0.73 | .465 |
| Research experience | No (ref: yes) | –0.13 | 0.12 | –.09 | –1.05 | .295 |
| Education on nursing management competency | No (ref: yes) | –0.14 | 0.10 | –.10 | –1.35 | .179 |
| Nursing environment | 0.41 | 0.10 | .33 | 4.27 | <.001 |
| Domain | Theme | Category | Subcategory | Quotes |
|---|---|---|---|---|
| Facilitators | Learning and organizational support as a foundation for nursing management competency development | Learning efforts for growth | Expansion of role perception and growth through education and practice experiences | During the graduate-level advanced practice nurse course, I received specialized education that made tasks such as statistical data analysis and report preparation more manageable (Participant19) |
| Self-development and adaptation to change | I believe continuous self-development is essential, because policies and social trends constantly change, and without keeping pace, it becomes very difficult to perform our work (Participant18) | |||
| Organizational support for education and learning | Professional development through specialized education and supervision | We receive weekly expert supervision, which has been highly beneficial (Participant20) | ||
| Application of nursing management competency through the integration of field-oriented initiatives and practical experience | Proactive practical leadership | Problem-solving leadership | The EMR system was prone to medication errors, so I suggested improvements to make it more user-friendly and to prevent errors in the medication return process (Participant17) | |
| Flexible leadership according to situations | I believe I exercised both a supportive, collaborative leadership style and a top-down leadership approach (Participant4) | |||
| Leadership through persuasion and direction | To ensure appropriate care, we had to present accreditation standards, but beyond that, we also needed to encourage and persuade others to collaborate (Participant4) | |||
| Leadership based on a sense of responsibility | I felt it was not about highlighting myself, but about demonstrating how well my team had performed, which required the presenter to be fully familiar with the content (Participant8) | |||
| Practical leadership in the process of system building | I participated in opening the emergency department and helped establish admission procedures and processes for patient history and comorbidity management (Participant17) | |||
| Diverse practical experiences | Integration of clinical, administrative, and community practice experiences | Field experience was very important. Working both in a hospital and at a community center helped me when engaging with clients (Participant18) | ||
| Professional competence grounded in practice and knowledge | My long clinical nursing experience, especially in communication and interpersonal skills, provided a foundation that strengthened my professional competence (Participant20) | |||
| Nursing management practice through interaction and collaboration | Interaction between leadership and followership | Acceptance of opinions through the balance of leadership and followership | When an experienced nurse suggested equipment use, it was accepted, showing the leader’s followership (Participant1) | |
| Leader-promoted growth atmosphere | What I valued in my supervisor was their desire to grow together with colleagues, as shown by their consistent dedication to study (Participant10) | |||
| Supervisory leadership and guidance | Having a good supervisor from whom I could seek advice was highly beneficial to me (Participant13) | |||
| Complementary collaboration | Collaboration and communication for common goals | Many new ideas emerged through discussions with colleagues about what to propose (Participant9) | ||
| Complementary teamwork through flexible roles | I believe teamwork is crucial; even when work is difficult, supportive colleagues help us move forward together (Participant18) | |||
| Barriers | Limitations arising from individual passivity and resistance to change | Individualism and passive participation | Weakening of team-based collaboration due to individualistic roles | They made adjustments for their own convenience, but when I was very busy, there was no consideration for my situation (Participant10) |
| Hindrance to collaboration from passivity and responsibility avoidance | A passive organizational culture has formed, leading people to refrain from sincere participation (Participant4) | |||
| Resistance to change | Demotivation from excessive stability | Motivation is lacking because our positions are relatively secure (Participant3) | ||
| Emotional exhaustion and frustration in change attempts | After repeated setbacks in such processes, I eventually found myself giving up (Participant18) | |||
| Conflicts between adherence to routines and change proposals | I hoped to try a new way, but senior staff were accustomed to old practices and could not recognize whether the suggestion was good or not (Participant6) | |||
| Limitations of repeated formal improvement activities | Repeatedly handling things in such a formal manner made us think it was not important and fall into the mindset of ‘this level is good enough’ (Participant6) | |||
| Structural and institutional constraints within the organization | Hierarchical organizational climate | Vertical communication structure | When I suggested a better way of doing things, if my superior simply said ‘no,’ that was the end of it (Participant2) | |
| Hierarchy-centered, rigid organizational culture | It feels like a vertical structure, which results in a significant lack of sense of solidarity (Participant9) | |||
| Inefficient human resource management system | Role overlap and workload burden from staff shortages | If staffing were sufficient, nurses would have more time with patients, allowing for more opportunities for interviews (Participant6) | ||
| Limited growth opportunities due to restricted personnel mobility | Opportunities for nurses to develop in national hospitals are quite limited, and experiences are insufficient (Participant1) | |||
| Constraints on leadership execution from mismatched rank and responsibility | The team leader seems to carry most of the work and responsibility, yet is largely excluded from authority (Participant20) | |||
| Limited reward and promotion system | Lack of recognition and rewards for performance and effort | Promotions and performance evaluations should differentiate between those who make an effort and those who do not (Participant14) | ||
| Seniority-based promotion and absence of diversified evaluation systems | Motivation declines because, regardless of effort, recognition is difficult when advancement is determined by seniority (Participant6) | |||
| Demotivation due to mismatch between work and rewards | Nurses handle a wide range of tasks, such as managing medications and conducting interviews, yet in the public service system, salaries remain the same even for supportive roles, as pay is based on grade and seniority (Participant11) | |||
| Inefficient work processes | Nurses’ disproportionate responsibility for interventions and communication | We ended up relaying messages to physicians, creating unnecessary back-and-forth communication (Participant11) | ||
| Inefficient task allocation entrenched by convention | My predecessor handled tasks haphazardly, and I had no choice but to follow the same way (Participant12) | |||
| Inefficiency from unaddressed field improvement demands | Even when frontline nurses propose improvement ideas, they are rarely adopted by the EMR team (Participant17) | |||
| Lack of guidance and mentoring system | Limited competency growth due to lack of role models | There should be someone to provide mentoring or serve as a role model, but currently there is no one (Participant1) | ||
| Difficulties in adaptation and performance from insufficient guidance | Most of the time, I had to figure things out on my own (Participant17) | |||
| Constraints on nursing management practice due to insufficient resources, collaboration, and educational systems | Rigid administrative structure and resource imbalance | Barriers to project implementation from policy and administrative procedures | There are many bureaucratic barriers to flexible project implementation, leading to unnecessary administrative procedures (Participant20) | |
| Shortage of resources and material support | When we requested necessary supplies, management dismissed it as too costly and told us to manage with what we already had (Participant1) | |||
| Lack of recognition of nursing expertise and limited interprofessional interaction | Limited opportunities for nurse participation in collaboration | There are too few opportunities to communicate with other departments or healthcare professionals (Participant1) | ||
| Lack of trust and recognition of nursing roles | There appears to be a highly hierarchical relationship between doctors and nurses, with poor communication (Participant10) | |||
| Insufficient organizational support for education and learning | Lack of diversity and practical applicability in education | Nurses have limited opportunities to gain financial experience, yet such knowledge is essential to understand the institution’s overall operations (Participant14) | ||
| Absence of knowledge-sharing and learning culture within the organization | The public hospital system has limitations in fostering a learning culture (Participant4) | |||
| Lack of systematic education and practice opportunities for strengthening administrative competence | The work gap was too large; after moving from patient care to administration, I was asked to draft a plan but could not understand it and found communication difficult (Participant10) |
| Nursing management process | Competencies (no. of items) | |
|---|---|---|
| Original version | Revised version | |
| Planning | Vision building (3) | Vision building (2) |
| Planning (3) | Planning (3) | |
| Analysis (4) | Analysis (4) | |
| Budget & fiscal management (4) | Budget & fiscal management (3) | |
| Decision-making (3) | Decision-making (3) | |
| Business & marketing (4) | Business & marketing (2) | |
| Organizing | Organization management (6) | Organization management (4) |
| Innovation & change management (5) | Innovation & change management (3) | |
| Human resources management | Staffing management (8) | Staffing management (5) |
| Human resources development & staff education (8) | Human resources development & staff education (7) | |
| Directing | Leadership (5) | Leadership (4) |
| Professionalism (4) | Professionalism (4) | |
| Nursing ethics & law (5) | Nursing ethics & law (4) | |
| Communication & interpersonal relationships (10) | Communication & interpersonal relationships (7) | |
| Community relationships (2) | - | |
| Cooperation & mediation (5) | Cooperation & mediation (4) | |
| Motivation (2) | Motivation (2) | |
| Problem-solving (5) | Problem-solving (4) | |
| Conflict management (2) | Conflict management (2) | |
| Negotiation (3) | Negotiation (2) | |
| Customer orientation (4) | Customer orientation (4) | |
| Self-management (5) | Self-management (5) | |
| Controlling | Quality improvement (3) | Quality improvement (3) |
| Development of nursing standard (3) | Development of nursing standard (3) | |
| Nursing practice (7) | Nursing practice (7) | |
| Resource management (3) | Resource management (2) | |
| Patient safety & infection management (6) | Patient safety & infection management (6) | |
| Information management (7) | Information management (6) | |
| Accreditation preparation (3) | Accreditation preparation (2) | |
| Performance management (6) | Performance management (6) | |
| Total | 30 competencies (138) | 29 competencies (113) |
| Category | Quantitative results | Qualitative results | Integration |
|---|---|---|---|
| Nursing work environment | • Perceived the nursing work environment was positively associated with nursing management competency performance | • Hierarchical organizational climate, rigid human resource, reward, and work systems, and insufficient mentoring limited nurses’ initiative, management-related role performance, and growth opportunities | • Organizational climate, system flexibility, resource availability, collaboration, and educational and mentoring support together constitute the nursing work environment, which in turn shaped nurses’ initiative, nursing management competency performance, and professional growth |
| • Administrative-centered procedures, insufficient material support, limited interprofessional collaboration, lack of recognition of nursing professionalism, and inadequate educational systems hindered nursing management competency development and professional growth | |||
| Clinical and professional experience | • Years of clinical experience were not significantly associated with nursing management competency | • Integration of clinical, administrative, and community practice experiences enhanced nurses’ practical understanding of their professional work, as well as their initiative | • Although total years of experience were not significant, diverse, and integrated professional experiences contributed meaningfully to nursing management competency development. |
| Education and learning support | • Educational level and prior nursing management competency–related education were not significantly associated with nursing management competency performance | • Individual learning efforts and organizational support for education served as a foundation for professional growth | • Formal education alone was insufficient; continuous learning and institutional educational support played critical roles in strengthening nursing management competencies |
Table 1. Differences in nursing management competency performance according to general characteristics (N=162)
1,2,3,4 in the last column represent the subgroup order (from the first to the last) for each variable in the post-hoc analysis. SD, standard deviation. a)By Scheffé test. b)By Welch test.
Table 2. Analysis of importance, performance, and needs of nursing management competencies (N=162)
Quadrant I: high importance/high performance; Quadrant II: high importance/low performance; Quadrant III: low importance/low performance; Quadrant IV: low importance/high performance. HH, high discrepancy/high importance; HL, high discrepancy/low importance; IPA, importance performance analysis; LF, locus for focus; LH, low discrepancy/high importance; LL, low discrepancy/low importance; SD, standard deviation. Priority competency items.
Table 3. Factors influencing the performance of nursing management competencies (N=162)
R²=.34, adjusted R²=.30, F=8.73, Ref, reference; SE, standard error.
Table 4. Facilitators and barriers of nursing management competency
The original version of nursing management competencies was derived from Kang and Kim [

