 Submit an article
Submit an article
Articles
- Page Path
- HOME > J Korean Acad Nurs > Volume 56(1); 2026 > Article
-
Research Paper
- Development and psychometric testing of the Perceived Postoperative Care Competency Scale for Nursing Students: a methodological study
-
Perihan Şimşek1
 , Gül Çakir Özmen2, Melek Ertürk Yavuz3, Sema Koçan4, Dilek Çilingir2
, Gül Çakir Özmen2, Melek Ertürk Yavuz3, Sema Koçan4, Dilek Çilingir2 -
Journal of Korean Academy of Nursing 2026;56(1):81-97.
DOI: https://doi.org/10.4040/jkan.25123
Published online: February 24, 2026
1Department of Emergency Aid and Disaster Management, Faculty of Applied Science, Trabzon University, Trabzon, Türkiye
2Department of Nursing, Faculty of Health Science, Karadeniz Technical University, Trabzon, Türkiye
3Department of Nursing, Faculty of Health Science, Artvin Çoruh University, Artvin, Türkiye
4Department of Nursing, Faculty of Health Science, Recep Tayyip Erdoğan University, Rize, Türkiye
- Corresponding author: Perihan Şimşek Trabzon University, Söğütlü, Adnan Kahveci Boulevard, 61335 Akçaabat, Trabzon, Türkiye E-mail: psimsek19@hotmail.com
• Received: August 28, 2025 • Revised: November 30, 2025 • Accepted: January 19, 2026
© 2026 Korean Society of Nursing Science
This is an Open Access article distributed under the terms of the Creative Commons Attribution NoDerivs License (http://creativecommons.org/licenses/by-nd/4.0) If the original work is properly cited and retained without any modification or reproduction, it can be used and re-distributed in any format and medium.
- 1,760 Views
- 164 Download
Abstract
-
Purpose
- To improve the quality of postoperative care and promote recovery after surgery, it is important that nursing education is competency-based and that competency assessment is an integral part of the educational process. The purpose of this study was to develop a tool to evaluate nursing students’ perceived competence in postoperative care.
-
Methods
- This cross-sectional methodological study followed DeVellis’s scale development steps and was conducted between December 2022 and March 2023. In this study, 892 students were invited and 703 responded. After exclusions, data from 645 students were analyzed to examine the psychometric structure of the scale using exploratory factor analysis (n=327) and confirmatory factor analysis (n=318). Reliability was assessed by calculating Cronbach’s α coefficients and by test–retest measurement (n=46).
-
Results
- The proposed scale was confirmed to consist of five factors and 28 items (χ2/degrees of freedom=2.25, root mean square error of approximation=.06, normed fit index=.90, and goodness-of-fit index=.85). Cronbach’s α was .97 for the total scale. The data demonstrated high test–retest stability (intraclass correlation coefficient=.88). The scale developed and psychometrically tested in this study revealed a five-factor structure: legal responsibilities and ethical principles (seven items), postoperative nursing care (seven items), interpersonal relations and communication (four items), leadership (six items), and education and professional development (four items).
-
Conclusion
- The scale, which demonstrated very good psychometric properties, would be helpful in assessing perceived postoperative nursing competence among nursing students. This may help students graduate with the necessary knowledge and skills required for postoperative care. However, further research involving larger samples and more diverse cultural contexts is needed to enhance the generalizability of the scale.
Introduction
Methods
1) Step 1: clearly defining the construct to be assessed
2) Step 2: generating a pool of items
3) Step 3: specifying the measurement format
4) Step 4: obtaining expert review of the initial items
5) Step 5: considering inclusion of validation items
6) Step 6: conducting a pilot test with a sample
7) Step 7: analyzing and refining the items/evaluate the items
(1) Item analysis
(2) Exploratory factor analysis
(3) Confirmatory factor analysis
(4) Reliability
8) Step 8: Optimizing the scale length
Results
1) Sample for EFA
2) Sample for CFA
Discussion
Conclusion
-
Conflicts of Interest
No potential conflict of interest relevant to this article was reported.
-
Acknowledgements
None.
-
Funding
None.
-
Data Sharing Statement
Please contact the corresponding author for data availability.
-
Author Contributions
Conceptualization or/and Methodology: PŞ, DÇ. Data curation or/and Analysis: PŞ, GÇÖ, SK, MEY. Funding acquisition: none. Investigation: PŞ, GÇÖ, SK, MEY. Project administration or/and Supervision: PŞ, DÇ. Resources or/and Software: none. Validation: PŞ, DÇ. Visualization: PŞ. Writing: original draft or/and Review & Editing: PŞ, GÇÖ, SK, MEY, DÇ. Final approval of the manuscript: all authors.
Article Information
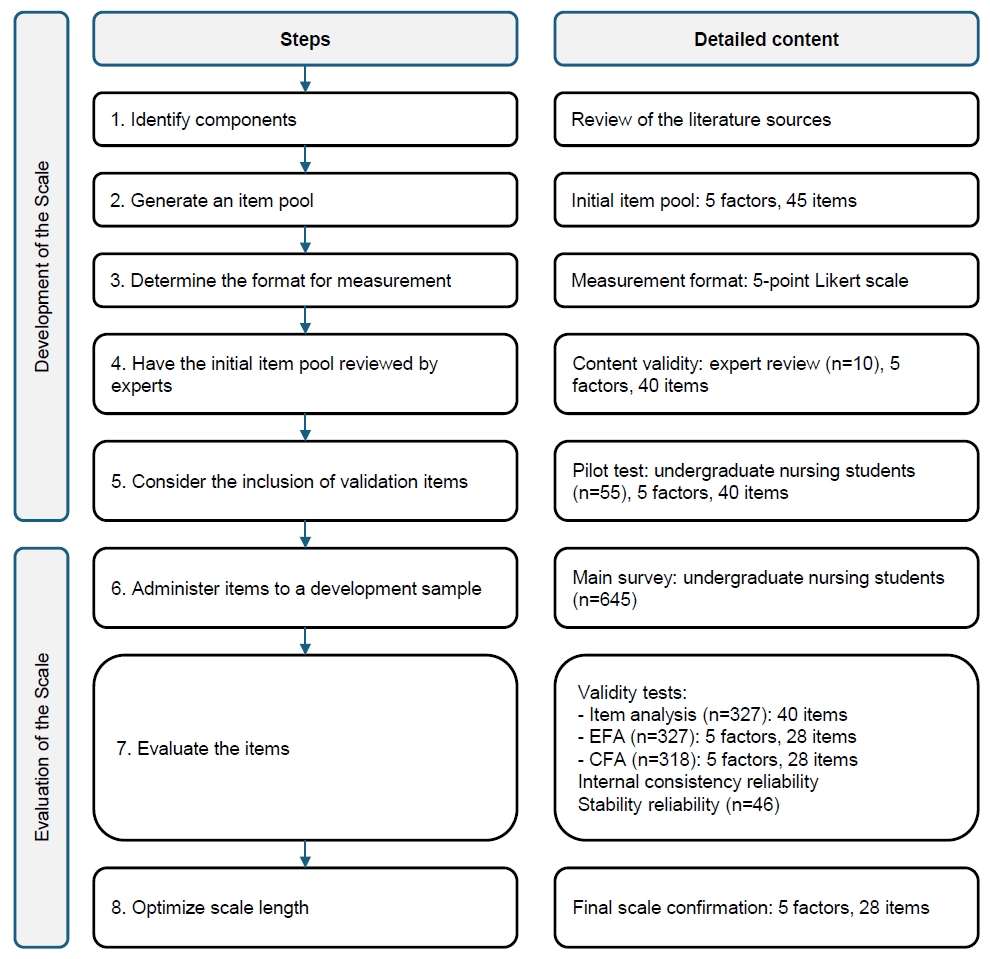
Fig. 2.Confirmatory factor analysis. F1: legal responsibilities and ethical principles, F2: postoperative nursing care, F3: interpersonal relations and communication, F4: leadership, F5: education and professional development. χ2=750.168; p=.000; degrees of freedom (df)=333; χ2/df=2.253; goodness-of-fit index=.846; root mean square error of approximation=.063; comparative fit index=.942; Tucker-Lewis index=.934; normed fit index=.901.
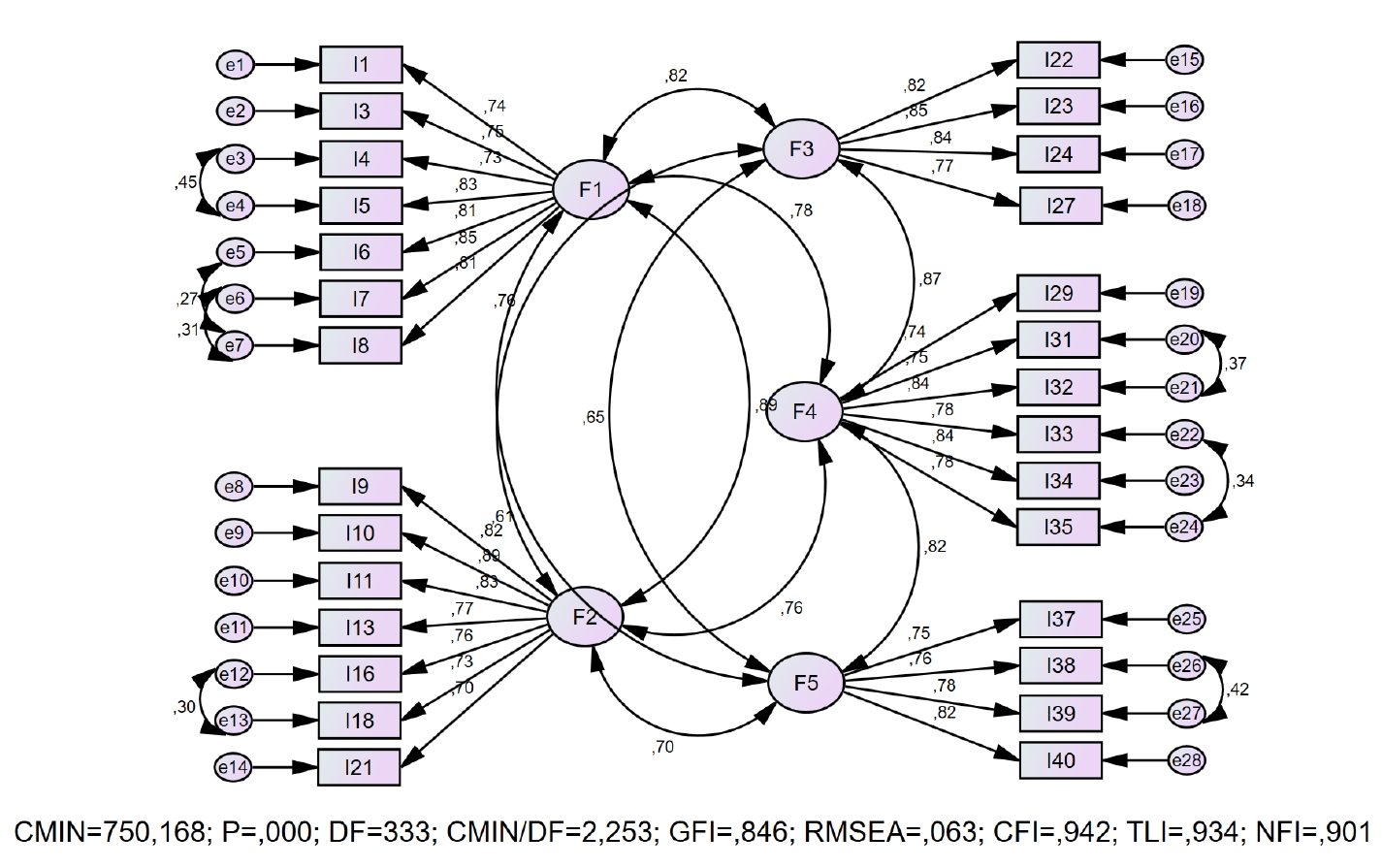
Table 1.Descriptive statistics (N=327)
Table 2.Factor loadings according to EFA (N=327)
Table 3.Stability reliability (N=46)
- 1. Rothrock JC. Alexander’s care of the patient in surgery. Elsevier Health Sciences; 2022.
- 2. Dencker EE, Bonde A, Troelsen A, Varadarajan KM, Sillesen M. Postoperative complications: an observational study of trends in the United States from 2012 to 2018. BMC Surg. 2021;21(1):393. https://doi.org/10.1186/s12893-021-01392-zArticlePubMedPMC
- 3. Qureshi IP, Qureshi S, Modi V. Study of early post-operative complications in relation to nature of anaesthesia and type of surgery. Int Surg. 2018;5(8):2827-2835. https://doi.org/10.18203/2349-2902.isj20183199Article
- 4. Benner P. From novice to expert. Am J Nurs. 1982;82(3):402-407. https://doi.org/10.1097/00000446-198282030-00004ArticlePubMed
- 5. Liu Y, Aungsuroch Y. Current literature review of registered nurses’ competency in the global community. J Nurs Scholarsh. 2018;50(2):191-199. https://doi.org/10.1111/jnu.12361ArticlePubMed
- 6. European Operating Room Nurses Association (EORNA). EORNA Framework for perioperative nurse competencies [Internet]. EORNA; 2009 [cited 2023 Jan 8]. Available from: https://eorna.eu/competencies/
- 7. European Operating Room Nurses Association (EORNA). EORNA common core curriculum for perioperative nursing [Internet]. EORNA; 2019 [cited 2024 Jun 1]. Available from: https://eorna.eu/eorna-common-core-curriculum-for-perioperative-nursing-third-edition-2019/
- 8. Kaldal MH, Conroy T, Feo R, Grønkjaer M, Voldbjerg SL. Umbrella review: Newly graduated nurses’ experiences of providing direct care in hospital settings. J Adv Nurs. 2023;79(6):2058-2069. https://doi.org/10.1111/jan.15434ArticlePubMed
- 9. Wallander Karlsen MM, Sørensen AL, Finsand C, Sjøberg M, Lieungh M, Stafseth SK. Combining clinical practice and education in critical care nursing: a trainee program for registered nurses. Nurs Open. 2023;10(6):3666-3676. https://doi.org/10.1002/nop2.1617ArticlePubMedPMC
- 10. Lewis LS, Rebeschi LM, Hunt E. Nursing education practice update 2022: competency-based education in nursing. SAGE Open Nurs. 2022;8:23779608221140774. https://doi.org/10.1177/23779608221140774ArticlePubMedPMC
- 11. Immonen K, Oikarainen A, Tomietto M, Kääriäinen M, Tuomikoski AM, Kaučič BM, et al. Assessment of nursing students’ competence in clinical practice: a systematic review of reviews. Int J Nurs Stud. 2019;100:103414. https://doi.org/10.1016/j.ijnurstu.2019.103414ArticlePubMed
- 12. Nehrir B, Vanaki Z, Mokhtari Nouri J, Khademolhosseini SM, Ebadi A. Competency in nursing students: a systematic review. Int J Travel Med Glob Health. 2016;4(1):3-11. https://doi.org/10.20286/ijtmgh-04013Article
- 13. Dermitzaki D, Haniotaki F, Fraidakis O, Papaioannou A, Askitopoulou H. Scale of quality of postoperative care. Eur J Anaesthesiol. 2000;17:19. https://doi.org/10.1097/00003643-200000002-00062Article
- 14. Gillespie BM, Polit DF, Hamlin L, Chaboyer W. Developing a model of competence in the operating theatre: psychometric validation of the perceived perioperative competence scale-revised. Int J Nurs Stud. 2012;49(1):90-101. https://doi.org/10.1016/j.ijnurstu.2011.08.001ArticlePubMed
- 15. Jeon Y, Lakanmaa RL, Meretoja R, Leino-Kilpi H. Competence assessment instruments in perianesthesia nursing care: a scoping review of the literature. J Perianesth Nurs. 2017;32(6):542-556. https://doi.org/10.1016/j.jopan.2016.09.008ArticlePubMed
- 16. Peñataro-Pintado E, Rodríguez-Higueras E, Llauradó-Serra M, Gómez-Delgado N, Llorens-Ortega R, Díaz-Agea JL. Development and validation of a questionnaire of the perioperative nursing competencies in patient safety. Int J Environ Res Public Health. 2022;19(5):2584. https://doi.org/10.3390/ijerph19052584ArticlePubMedPMC
- 17. Joo GE, Sohng KY. Development of nursing competence scale for graduating nursing students. J Korean Public Health Nurs. 2014;28(3):590-604. https://doi.org/10.5932/JKPHN.2014.28.3.590Article
- 18. Liou SR, Cheng CY. Developing and validating the Clinical Competence Questionnaire: a self-assessment instrument for upcoming baccalaureate nursing graduates. J Nurs Educ Pract. 2014;4(2):56-66. https://doi.org/10.5430/jnep.v4n2p56Article
- 19. Vallejo-Gómez L, Ruiz-Recéndiz M, Jiménez-Arroyo V, Alcántar-Zavala ML, Huerta-Baltazar MI. Instruments to measure nursing competencies: systematic review. Sanus. 2021;6:e198. https://doi.org/10.36789/revsanus.vi1.198Article
- 20. Gabbard T, Romanelli F. The accuracy of health professions students’ self-assessments compared to objective measures of competence. Am J Pharm Educ. 2021;85(4):8405. https://doi.org/10.5688/ajpe8405ArticlePubMedPMC
- 21. DeVellis RF. Scale development: theory and applications. SAGE Publications; 2003.
- 22. Nursing and Midwifery Council (NMC). Standards for competence for registered nurses [Internet]. NMC; 2010 [cited 2023 Jan 5]. Available from: https://www.nmc.org.uk/globalassets/sitedocuments/standards/nmc-standards-for-competence-for-registered-nurses.pdf
- 23. Wu XV, Enskär K, Lee CC, Wang W. A systematic review of clinical assessment for undergraduate nursing students. Nurse Educ Today. 2015;35(2):347-359. https://doi.org/10.1016/j.nedt.2014.11.016ArticlePubMed
- 24. European Operating Room Nurses Association (EORNA). EORNA framework for perioperative nurse competencies [Internet]. EORNA; 2019 [cited 2023 Jan 5]. Available from: https://eorna.eu/wp-content/uploads/2019/05/Competencies-brochure-final.pdf
- 25. Davis LL. Instrument review: getting the most from a panel of experts. Appl Nurs Res. 1992;5(4):194-197. https://doi.org/10.1016/S0897-1897(05)80008-4Article
- 26. Alpar R. Spor Sağlık ve Eğitim Bilimlerinden Örneklerle Uygulamalı İstatistik ve Geçerlik-Güvenirlik [Applied statistics and validity-reliability with examples from sports, health and educational sciences]. Detay Yayincilik; 2016.
- 27. Tavakol M, Wetzel A. Factor analysis: a means for theory and instrument development in support of construct validity. Int J Med Educ. 2020;11:245-247. https://doi.org/10.5116/ijme.5f96.0f4aArticlePubMedPMC
- 28. Anderson JC, Gerbing DW. The effect of sampling error on convergence, improper solutions, and goodness-of-fit indices for maximum likelihood confirmatory factor analysis. Psychometrika. 1984;49(2):155-173. https://doi.org/10.1007/BF02294170Article
- 29. Hu LT, Bentler PM. Cutoff criteria for fit indexes in covariance structure analysis: conventional criteria versus new alternatives. Struct Equ Modeling. 1999;6(1):1-55. https://doi.org/10.1080/10705519909540118Article
- 30. Marsh HW, Hau KT. Assessing goodness of fit: is parsimony always desirable? J Exp Educ. 1996;64(4):364-390. https://doi.org/10.1080/00220973.1996.10806604Article
- 31. Wheaton B, Muthen B, Alwin DF, Summers GF. Assessing reliability and stability in panel models. Sociol Methodol. 1977;8:84-136. https://doi.org/10.2307/270754Article
- 32. Jager J, Putnick DL, Bornstein MH. II. More than just convenient: the scientific merits of homogeneous convenience samples. Monogr Soc Res Child Dev. 2017;82(2):13-30. https://doi.org/10.1111/mono.12296ArticlePubMedPMC
- 33. Karagöz Y. SPSS 21.1 uygulamali biyoistatistik [SPSS 21.1 applied biostatistics]. Nobel Publishing and Distribution; 2014.
- 34. MRC Cognition and Brain Sciences Unit. Testing normality including skewness and kurtosis [Internet]. University of Cambridge; c2009 [cited 2026 Feb 2]. Available from: https://imaging.mrc-cbu.cam.ac.uk/statswiki/FAQ/Simon
- 35. Peterson RA. A meta-analysis of variance accounted for and factor loadings in exploratory factor analysis. Mark Lett. 2000;11(3):261-275. https://doi.org/10.1023/A:1008191211004Article
- 36. Hair JF, Black WC, Babin BJ, Anderson RE. Multivariate data analysis. 7th ed. Pearson; 2009.
- 37. Ciğerci Y, Yılmaz MA. Intraoperative patient care knowledge levels of operating room nurses: a case of Afyonkarahisar. Kocatepe Med J. 2022;23(2):152-159. https://doi.org/10.18229/kocatepetip.890328Article
- 38. Şimşek P, Özmen GÇ, Yavuz ME, Koçan S, Çilingir D. Exploration of nursing students’ views on the theory-practice gap in surgical nursing education and its relationship with attitudes towards the profession and evidence-based practice. Nurse Educ Pract. 2023;69:103624. https://doi.org/10.1016/j.nepr.2023.103624ArticlePubMed
- 39. Taşdemir N, Yavuz M. Family-centered approach in perioperative nursing. Ege Univ Fac Nurs J [Internet]. 2008 [cited 2026 Feb 2];24(1):91-99. Available from: https://dergipark.org.tr/tr/pub/egehemsire/article/635595
- 40. Dallı ÖE, Arkan B. Adaptation and assessment of the psychometric properties of the Turkish version of the nursing student competence scale. BMC Med Educ. 2025;25(1):324. https://doi.org/10.1186/s12909-025-06891-8ArticlePubMedPMC
- 41. Abuadas MH. The Arabic Nurse Professional Competence-Short Version Scale (NPC-SV-A): transcultural translation and adaptation with a cohort of Saudi nursing students. Healthcare (Basel). 2023;11(5):691. https://doi.org/10.3390/healthcare11050691ArticlePubMedPMC
- 42. Xu L, Nilsson J, Zhang J, Engström M. Psychometric evaluation of Nurse Professional Competence Scale-Short-form Chinese language version among nursing graduate students. Nurs Open. 2021;8(6):3232-3241. https://doi.org/10.1002/nop2.1036Article
- 43. Şimşek P, Özmen GÇ, Kemer AS, Aydin RK, Bulut E, Çilingir D. Development and psychometric testing of Perceived Preoperative Nursing Care Competence Scale for Nursing Students (PPreCC-NS). Nurse Educ Today. 2023;120:105632. https://doi.org/10.1016/j.nedt.2022.105632ArticlePubMed
- 44. Anema MG, McCoy JL. Competency based nursing education: guide to achieving outstanding learner outcomes. Springer Publishing Company; 2009.
- 45. Dikmen Y, Denat Y, Başaran H, Filiz NY. Hemşirelik öğrencilerinin öz etkililik-yeterlik düzeylerinin incelenmesi [Examination of self-efficacy levels of nursing students]. J Contemp Med. 2016;6(3):206-213. https://doi.org/10.16899/ctd.93945Article
- 46. American Association of Colleges of Nursing (AACN). Commission on Collegiate Nursing Education (CCNE): standards for accreditation of baccalaureate and graduate nursing programs [Internet]. AACN; 2024 [cited 2025 Nov 30]. Available from: https://www.aacnnursing.org
- 47. Lee BO, Liang HF, Chu TP, Hung CC. Effects of simulation-based learning on nursing student competences and clinical performance. Nurse Educ Pract. 2019;41:102646. https://doi.org/10.1016/j.nepr.2019.102646ArticlePubMed
- 48. Marshburn DM, Engelke MK, Swanson MS. Relationships of new nurses’ perceptions and measured performance-based clinical competence. J Contin Educ Nurs. 2009;40(9):426-432. https://doi.org/10.3928/00220124-20090824-02ArticlePubMed
- 49. Han Y, Kim JS, Seo Y. Cross-sectional study on patient safety culture, patient safety competency, and adverse events. West J Nurs Res. 2020;42(1):32-40. https://doi.org/10.1177/0193945919838990ArticlePubMed
- 50. Tajvidi M, Moghimi HS. The relationship between critical thinking and clinical competence in nurses. Strides Dev Med Educ. 2019;16(1):e80152. https://doi.org/10.5812/sdme.80152Article
References
Appendix
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
 ePub Link
ePub Link Cite
Cite- Figure
-
- We recommend
- Related articles
-
- Corrigendum: Psychometric testing of the Korean version of the Undergraduate Nursing Student Academic Satisfaction Scale: a methodological study
- Psychometric testing of the Korean version of the Undergraduate Nursing Student Academic Satisfaction Scale: a methodological study
- Reliability and validity of the Korean version of the Nurses Professional Values Scale-3 for nursing students: a methodological study
- Development of the Hybrid Clinical Practicum Environment Scale for Nursing Students
Development and psychometric testing of the Perceived Postoperative Care Competency Scale for Nursing Students: a methodological study
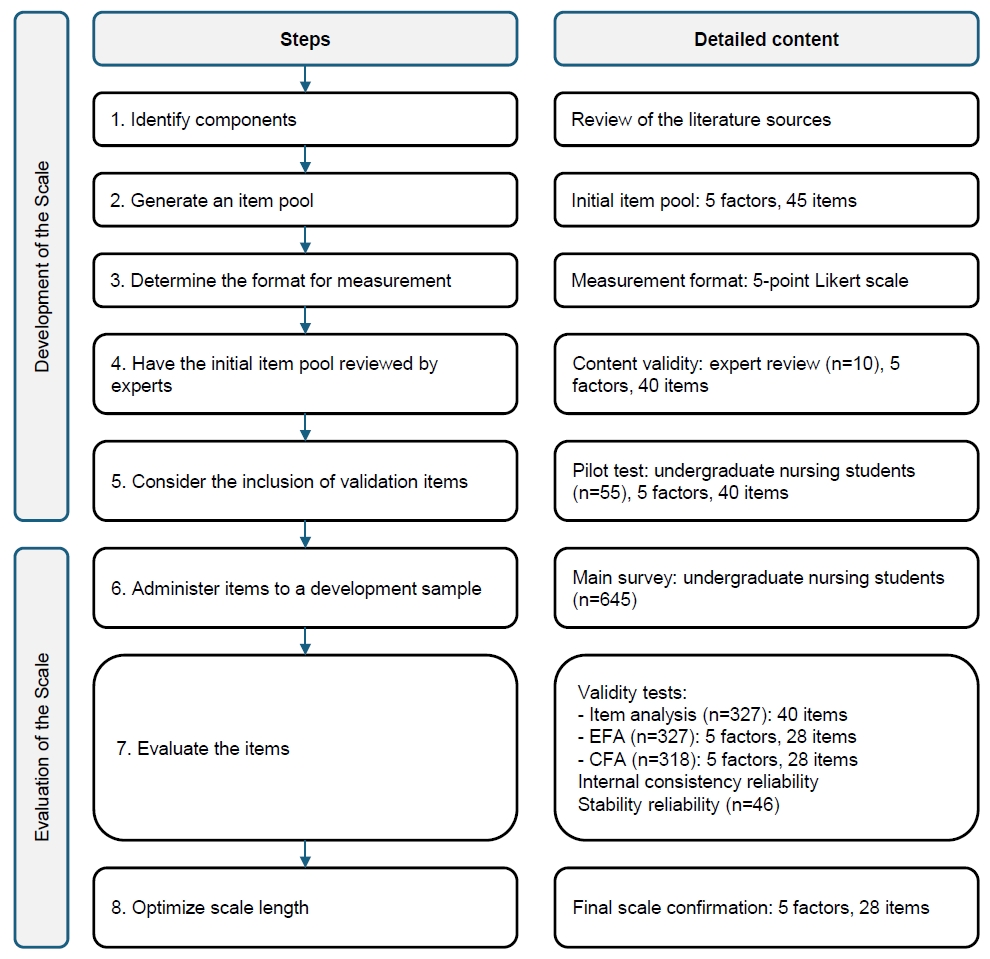
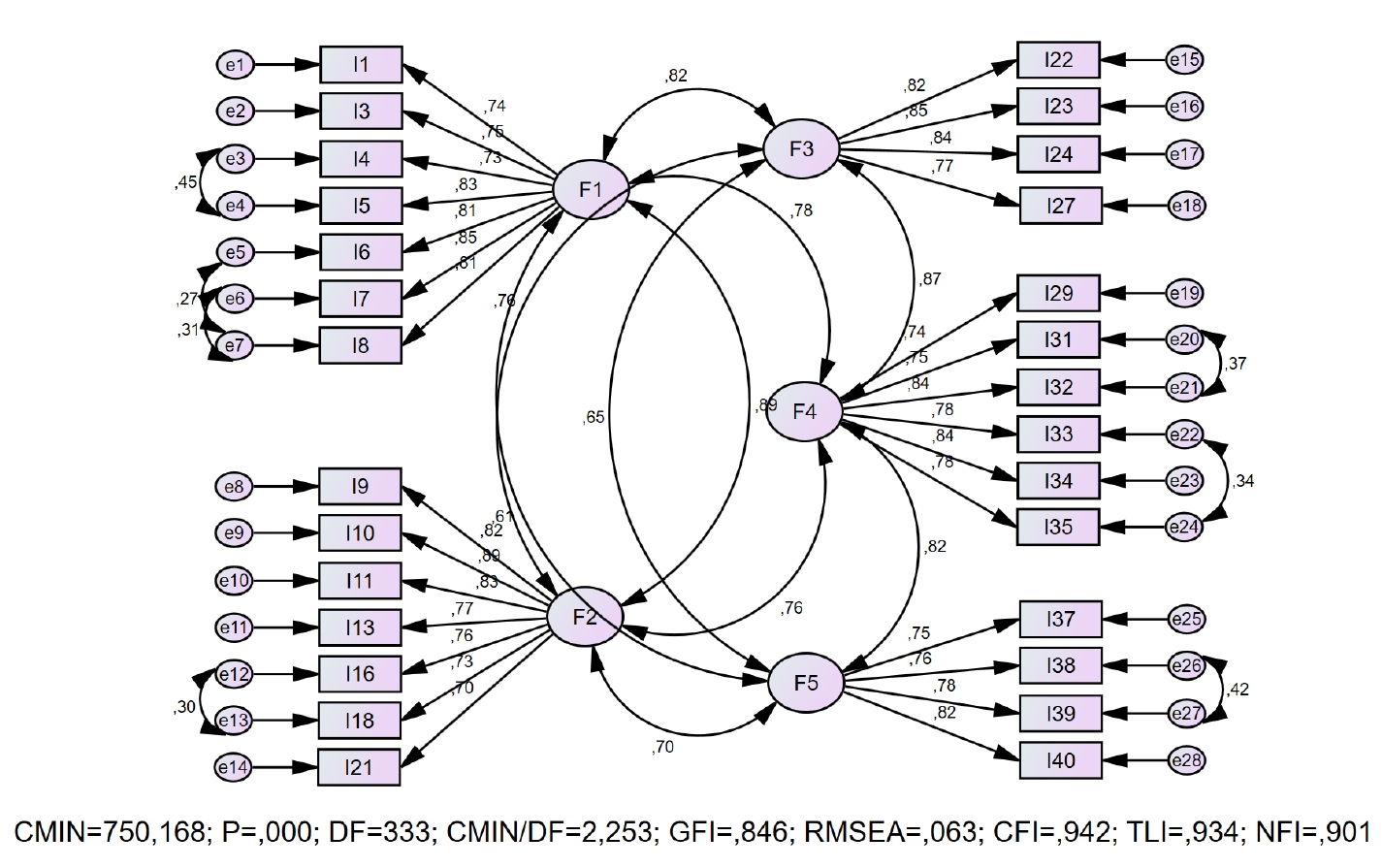
Fig. 1. Study flow diagram.
Fig. 2. Confirmatory factor analysis. F1: legal responsibilities and ethical principles, F2: postoperative nursing care, F3: interpersonal relations and communication, F4: leadership, F5: education and professional development. χ2=750.168; p=.000; degrees of freedom (df)=333; χ2/df=2.253; goodness-of-fit index=.846; root mean square error of approximation=.063; comparative fit index=.942; Tucker-Lewis index=.934; normed fit index=.901.
Fig. 1.
Fig. 2.
Development and psychometric testing of the Perceived Postoperative Care Competency Scale for Nursing Students: a methodological study
| No. | Item | Mean±SD | Corrected item-total correlation | Cronbach’s α if item deleted |
|---|---|---|---|---|
| I1 | I can comply with the basic ethical principles in postoperative nursing practices | 4.37±.70 | .52 | .96 |
| I3 | I can take responsibility for postoperative care practices | 4.32±.75 | .55 | .96 |
| I4 | I can consult health care professionals about postoperative care practices that are beyond my capacity | 4.66±.58 | .54 | .96 |
| I5 | I can ensure the confidentiality and security of patient information that I receive | 4.73±.52 | .52 | .96 |
| I6 | I can document my nursing practice in the postoperative period | 4.47±.66 | .54 | .96 |
| I7 | I can take measures to ensure patient safety in postoperative care | 4.59±.58 | .62 | .96 |
| I8 | I can use checklists to ensure patient safety in postoperative care | 4.5±.65 | .63 | .96 |
| I9 | I can carry out a physical assessment of the patient in the postoperative period | 4.42±.63 | .54 | .96 |
| I10 | I can provide postoperative nursing care according to relevant procedures and protocols | 4.36±.67 | .66 | .96 |
| I11 | I can provide patient-specific care using the nursing process in postoperative patient care | 4.41±.69 | .68 | .96 |
| I13 | I can apply evidence-based guidelines for surgical site skin care | 4.24±.76 | .60 | .96 |
| I16 | I can plan the necessary nursing care for fluid and electrolyte imbalances that may occur after surgery | 4.22±.71 | .64 | .96 |
| I18 | I can plan nursing care to prevent the development of deep vein thrombosis after surgery | 4.23±.77 | .63 | .96 |
| I21 | I can recognize emergencies that may occur in the postoperative period | 4.13±.73 | .63 | .96 |
| I22 | I can provide an appropriate communication environment for the patient to express their concerns by using effective communication techniques | 4.39±.73 | .68 | .96 |
| I23 | I can use interpersonal communication skills to enhance the patient’s strategies for coping with postoperative anxiety | 4.32±.69 | .69 | .96 |
| I24 | I can provide positive communication and co-operation with patients and their relatives to increase participation in patient care | 4.46±.67 | .71 | .96 |
| I27 | During the postoperative care process, I avoid judgmental attitudes and try to understand patients and their relatives | 4.52±.65 | .57 | .96 |
| I29 | I can take responsibility for my own professional development in postoperative practices | 4.35±.76 | .65 | .96 |
| I31 | I strive to contribute to the self-development of my colleagues in postoperative nursing | 4.41±.69 | .65 | .96 |
| I32 | I can contribute to harmonious and organized work of my fellow students in the postoperative care units | 4.49±.65 | .61 | .96 |
| I33 | I can consult with members of the surgical team to learn what I do not know about postoperative care | 4.6±.60 | .66 | .96 |
| I34 | I can share my knowledge and experience of postoperative care with my peers and nurses | 4.5±.70 | .71 | .96 |
| I35 | I can benefit from the knowledge and experience of the surgical team members | 4.62±.57 | .68 | .96 |
| I37 | I can follow current research in postoperative care | 4.23±.77 | .58 | .96 |
| I38 | I try to contribute to the development of new technological products and equipment to improve postoperative care | 4.04±.90 | .47 | .96 |
| I39 | I try to contribute to scientific research regarding postoperative care | 4.04±.89 | .50 | .96 |
| I40 | I can benefit from technological developments to increase the effectiveness of postoperative care | 4.35±.71 | .62 | .96 |
| Items | CVI | Communalities | Factors | |||||
|---|---|---|---|---|---|---|---|---|
| Initial | Extraction | 1 | 2 | 3 | 4 | 5 | ||
| I1 | 1 | .45 | .36 | .47 | ||||
| I3 | 1 | .49 | .43 | .44 | ||||
| I4 | 1 | .54 | .50 | .57 | ||||
| I5 | .90 | .54 | .54 | .68 | ||||
| I6 | 1 | .49 | .44 | .58 | ||||
| I7 | 1 | .62 | .60 | .66 | ||||
| I8 | .80 | .62 | .59 | .64 | ||||
| I9 | .90 | .45 | .41 | .47 | ||||
| I10 | .90 | .61 | .58 | .51 | ||||
| I11 | .90 | .56 | .54 | .40 | ||||
| I13 | 1 | .51 | .47 | .45 | ||||
| I16 | .80 | .52 | .49 | .44 | ||||
| I18 | .80 | .58 | .47 | .44 | ||||
| I21 | .90 | .58 | .52 | .52 | ||||
| I22 | 1 | .76 | .76 | –.81 | ||||
| I23 | 1 | .73 | .66 | –.64 | ||||
| I24 | 1 | .71 | .70 | –.65 | ||||
| I27 | .80 | .57 | .53 | –.46 | ||||
| I29 | .90 | .59 | .53 | –.43 | ||||
| I31 | 1 | .69 | .56 | –.59 | ||||
| I32 | 1 | .69 | .59 | –.73 | ||||
| I33 | .80 | .67 | .64 | –.67 | ||||
| I34 | 1 | .67 | .64 | –.61 | ||||
| I35 | 1 | .70 | .66 | –.61 | ||||
| I37 | .80 | .64 | .59 | .62 | ||||
| I38 | 1 | .62 | .67 | .85 | ||||
| I39 | 1 | .67 | .64 | .79 | ||||
| I40 | .90 | .60 | .50 | .45 | ||||
| Sub-dimensions | Mean±SD | t | p | ICC | |
|---|---|---|---|---|---|
| Test | Re-test | ||||
| F1 | 30.87±3.83 | 30.24±3.63 | 1.73 | .090 | .87 |
| F2 | 33.33±10.76 | 32.80±11.14 | .86 | .390 | .96 |
| F3 | 17.50±2.47 | 17.17±2.26 | 1.00 | .320 | .72 |
| F4 | 26.61±3.38 | 25.85±3.35 | 1.70 | .095 | .73 |
| F5 | 16.61±2.58 | 16.04±3.00 | 1.42 | .162 | .69 |
| Total | 124.91±16.56 | 122.11±17.39 | 1.74 | .088 | .88 |
Table 1. Descriptive statistics (N=327)
SD, standard deviation.
Table 2. Factor loadings according to EFA (N=327)
F1: legal responsibilities and ethical principles, F2: postoperative nursing care, F3: interpersonal relations and communication, F4: leadership, F5: education and professional development. CVI, content validity index; EFA, exploratory factor analysis.
Table 3. Stability reliability (N=46)
ICC, intraclass correlation coefficient; SD, standard deviation.

