 Submit an article
Submit an article
Articles
- Page Path
- HOME > J Korean Acad Nurs > Volume 50(4); 2020 > Article
- Original Article Effectiveness of Multi Interventional Package on Selected Parameters of Metabolic Syndrome among Women - A Pilot Study
- Attonassary Jose Elizabeth, Swaminathan Aruna, Parayidathil Joseph Mercy
-
Journal of Korean Academy of Nursing 2020;50(4):523-532.
DOI: https://doi.org/10.4040/jkan.20012
Published online: August 31, 2020
1Department of Research, Saveetha University, Chennai, India
2Medical Surgical Nursing, Saveetha College of Nursing, SIMATS, Chennai, India
3Center for Medical Simulation, Kerala University of Health Sciences, Thrissur, India
2Medical Surgical Nursing, Saveetha College of Nursing, SIMATS, Chennai, India
3Center for Medical Simulation, Kerala University of Health Sciences, Thrissur, India
- 1,320 Views
- 28 Download
- 0 Crossref
- 0 Scopus
Abstract
Purpose
The purpose of the study was to compare the effectiveness of multi interventional package (MIP) and lifestyle interventions (LI) on physiological parameters of women with metabolic syndrome, to compare the effectiveness of MIP and LI on biochemical parameters of women with metabolic syndrome and to compare the effectiveness of MIP and LI on socio-psychological parameters of women with metabolic syndrome.
Methods
A quasi experimental nonequivalent control group design with two experimental groups and one control group was used to collect data from 60 self-help group women. Samples were selected by multistage sampling. Reflexology foot massage, dietary modification, moderate intensity exercise and structured education were given to MIP group and dietary modification, moderate intensity exercise and structured education were given to LI group for 12 weeks. Control group received routine care. Demographic and clinical data sheets were used to collect basic information. Knowledge was assessed by a knowledge questionnaire. Physiological (weight, body mass index, waist circumference and blood pressure) and biochemical parameters (HDL, triglycerides and FBS) were assessed before and after the intervention.
Results
The study found significant change in the physiological and biochemical parameters of metabolic syndrome as well as knowledge among the MIP group and LI group compared to the control group (p < .001).
Conclusion
MIP and LI are effective in controlling the parameters of metabolic syndrome. Hence the guidance may be provided to women with metabolic syndrome for adopting necessary lifestyle changes as well as reflexology foot massage to control the physiological and biochemical parameters of metabolic syndrome.
J Korean Acad Nurs. 2020 Aug;50(4):523-532. English.
Published online Aug 31, 2020.
https://doi.org/10.4040/jkan.20012
Published online Aug 31, 2020.
https://doi.org/10.4040/jkan.20012
© 2020 Korean Society of Nursing Science
Original Article
Effectiveness of Multi Interventional Package on Selected Parameters of Metabolic Syndrome among Women: A Pilot Study
Abstract
Purpose
The purpose of the study was to compare the effectiveness of multi interventional package (MIP) and lifestyle interventions (LI) on physiological parameters of women with metabolic syndrome, to compare the effectiveness of MIP and LI on biochemical parameters of women with metabolic syndrome and to compare the effectiveness of MIP and LI on socio-psychological parameters of women with metabolic syndrome.
Methods
A quasi experimental nonequivalent control group design with two experimental groups and one control group was used to collect data from 60 self-help group women. Samples were selected by multistage sampling. Reflexology foot massage, dietary modification, moderate intensity exercise and structured education were given to MIP group and dietary modification, moderate intensity exercise and structured education were given to LI group for 12 weeks. Control group received routine care. Demographic and clinical data sheets were used to collect basic information. Knowledge was assessed by a knowledge questionnaire. Physiological (weight, body mass index, waist circumference and blood pressure) and biochemical parameters (HDL, triglycerides and FBS) were assessed before and after the intervention.
Results
The study found significant change in the physiological and biochemical parameters of metabolic syndrome as well as knowledge among the MIP group and LI group compared to the control group (p < .001).
Conclusion
MIP and LI are effective in controlling the parameters of metabolic syndrome. Hence the guidance may be provided to women with metabolic syndrome for adopting necessary lifestyle changes as well as reflexology foot massage to control the physiological and biochemical parameters of metabolic syndrome.
Keywords
Obesity; Hyperlipidemia; Hypertension; Metabolic Syndrome
INTRODUCTION
Metabolic syndrome (MS) is a complex pathophysiologic state that originates from an imbalance of calorie intake and energy expenditure. It is also affected by the genetic makeup of the individual, sedentary lifestyle, quality and composition of food and microbes in the gastrointestinal tract [1]. As per the National Cholesterol Education Program Adult Treatment Panel III (NCEP-ATP III), to diagnose metabolic syndrome, three or more criteria among the following should be present; abdominal obesity (waist circumference > 102 cm in men and > 88 cm in women), hypertriglyceridemia (≥ 150 mg/dl), low high density lipoprotein (HDL) cholesterol (< 40 mg/dl in men and < 50 mg/dl in women), high blood pressure (≥ 130/85 mmHg) and high fasting blood sugar (FBS) (≥ 110 mg/dl) [2]. In India, prevalence of MS in the urban women population is very high (48.20%) as compared to men (16.31%) [3].
MS is a disorder characterized by a cluster of interconnected factors that increase the risk for cardiovascular atherosclerotic diseases and type 2 diabetes mellitus [4]. Due to its impact on health and financial implications, the mechanism that contributes to the pathogenesis of metabolic syndrome remains under intense investigation [5]. MS is a screening tool and it should be used to identify people at high risk of metabolic complications and cardiovascular diseases, so that further detailed investigations can be performed [6].
Some exceptional factors determine the prevalence and features of MS among women; pregnancy, gestational diabetes mellitus, history of preeclampsia and polycystic ovarian syndrome are considered as the contributing factors for MS among women whereas, lactation can decrease woman's risk for the development of MS [7]. The prevalence of MS increases with menopause. The progression from pre to post menopause is linked with the development of many features of the MS like increased central body fat, increased low-density lipoprotein (LDL) and triglycerides levels, reduced HDL, and increased glucose and insulin levels [8].
Reflexology is a type of massage that involves applying different amounts of pressure to the feet, hands and ears. It is based on a theory that these body parts are connected to certain organs and body systems. Applying pressure or massaging certain spots on the feet and hands, all other body parts could be revitalized [9]. Studies show that reflexology foot massage has a significant effect on blood pressure, lipoproteins and blood sugar levels. There are number of studies done on the effect of reflexology foot massage, dietary modifications, exercise and education on different aspects of metabolic syndrome [10] Investigator observed that emergence of MS among women is mainly in the middle age and control measures in this stage will be helpful to prevent the development of cardiovascular diseases and type 2 diabetes mellitus [11]. It will help to improve the quality of life of people in a developing country like India. Hence, it is decided to conduct the study among middle age women. The researcher also wanted to identify the impact of reflexology along with lifestyle intervention and decided to have two experimental groups and one control group. The statement of the problem was to assess the effectiveness of multi interventional package (MIP) and lifestyle interventions (LI) on physiological and biochemical parameters of metabolic syndrome among women. The purposes of this study were to (a) to compare the effectiveness of MIP and LI on physiological parameters of women with metabolic syndrome, (b) to compare the effectiveness of MIP and LI on biochemical parameters of women with metabolic syndrome, (c) to compare the effectiveness of MIP and LI on socio-psychological parameters of women with metabolic syndrome.
METHODS
1. Study design
A quantitative research approach was used to compare the effectiveness of LI and MIP on physiological, biochemical and socio psychological parameters of metabolic syndrome. A quasi experimental nonequivalent control group design was used in this study. The MIP group received reflexology foot massage sessions along with lifestyle interventions and the LI group received lifestyle interventions alone. No intervention was given to control group and were instructed to follow the routine care advised by the health care provider (Figure 1). The main intention was to find out the benefit of adding reflexology to lifestyle intervention in the outcomes. By including three groups comparison was done with the lifestyle intervention group as well as with the control group.
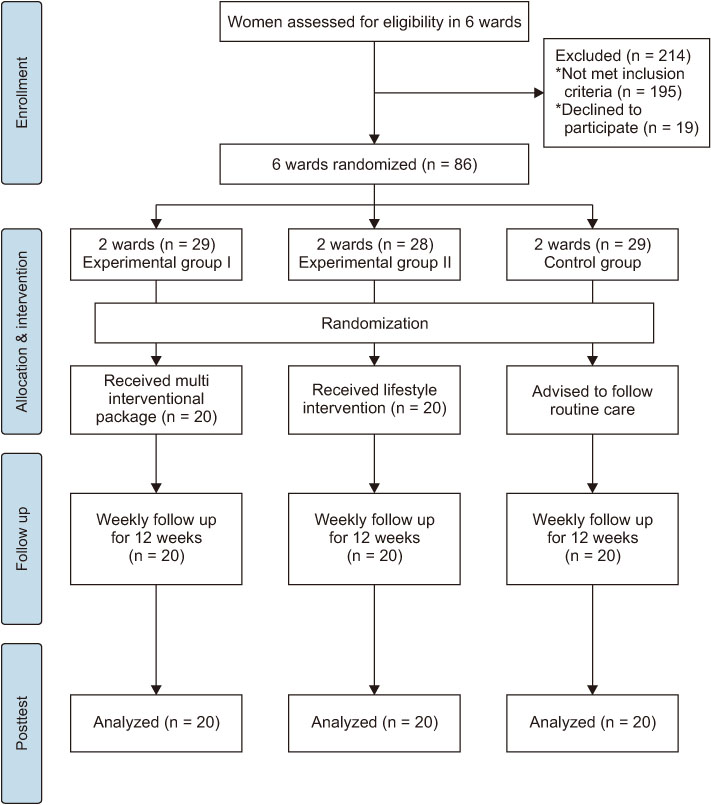
Figure 1
Flow diagram of the study.
2. Setting and samples
This study was conducted among self-help group women from six wards of two area development societies in a selected area in South India. As per the previous studies the minimum sample size for pilot trial is ≥ 55 [12]. Since it was a pilot study and there was no previous literature available regarding the same topic, we took 60 samples [13] by multistage sampling technique. 300 women from six wards of two area development societies were assessed for eligibility and among them 86 met the inclusion criteria. These six wards were randomly assigned into multi interventional package group (2 wards), lifestyle intervention group (2 wards) and control group (2 wards). Participants were assigned with random numbers and drawn the numbers from 1 to 20 using a computer generated random table. Inclusion criteria for the study were women belong to the age group of 35 to 55 years and meet any three of the following five criteria of metabolic syndrome such as waist circumference > 88 cm, high Blood pressure: SBP > 130 mmHg or DBP > 85 mmHg or on treatment for hypertension, high Fasting blood sugar > 100 mg/dl or on treatment for DM, HDL < 50 mg/dl, triglycerides > 150 mg/dl. Women who reported with a history of cardiac disease, renal disease, cancer, ligament injury, surgery in the leg, neurovascular problems, pregnancy, psychiatric disorders and severe cognitive impairment were excluded from the study.
3. Instruments/measurements
1) Socio-demographic and clinical information sheet
The data included the demographic and clinical variables of women consisting of age, marital status, education, occupation, monthly income, type of family, preferred food groups, lifestyle habits, menstruation, history of diabetes and hypertension during pregnancy, history of polycystic ovarian syndrome, history of oral contraceptive pill use, history of diabetes mellitus, history of hypertension and dyslipidemia.
2) Structured knowledge questionnaire
The structured questionnaire was developed by the researchers to determine the socio-psychological variable in terms ofknowledge of women regarding MS. It included 20 questions related to various aspects of metabolic syndrome like definition, etiology and risk factors, components and its preventive measures. Each right answer carries a score of “1” and wrong answers “0”. The reliability of the questionnaire was measured by Cronbach's alpha and the reliability index was .71 which indicated that the tool is reliable. Content validity of the questionnaire was determined according to clarity, relevancy and simplicity of each question from 10 experts in the fields of medicine, nursing, alternative medicine, nutritionists, physiotherapists and statisticians. Twenty questions with item content validity index more than .80 was included in the questionnaire. Scale content validity index was .90.
3) Physiological parameters
This includes bodyweight (kg), height (cm), BMI (kg/m2), waist circumference (cm) and blood pressure (mmHg). Weight was measured by a calibrated weighing scale (Samso sleek weighing scale, Central Denmark). Height was measured by using non-stretching inch tape without shoe heals touching the walls with the back in a straight position and heads to their normal anatomic position. BMI was calculated by the formula, weight/height (m2). BMI was scored as < 18.5 underweight, between 18.5 to 24.9 normal and ≥ 25 as overweight and obese. Waist circumference was measured with non-stretching tape placed on a horizontal line above the top of the iliac bone when the woman is standing with arms hanging down freely following a normal expiration. Systolic and diastolic BP were measured using a calibrated sphygmomanometer (Aneroid sphygmomanometer, Model No: CEO483, New Delhi, India) and stethoscope from the left arm in the sitting position. According to National Cholesterol Education Program-Adult Treatment Panel III criteria BP > 130/85 mmHg is considered as a criterion for metabolic syndrome [2].
4) Biochemical measurements
This includes fasting blood sugar (FBS) (mg/dl), HDL (mg/dl), and triglycerides (mg/dl). Biochemical measurements were done by collecting 10 ml of blood from the participants at 9 am after a 12 hour overnight fast. Triglycerides and FBS were tested by the Glycerol phosphate oxidase-peroxidase (GPO-POD) method and high density lipoprotein (HDL) using a homogenous method.
4. Interventions
Group I: MIP (reflexology foot massage, diet, exercise and education) was given to group I. Reflexology foot massage was given 30 minutes to areas specific to metabolic syndrome; lungs, thyroid, liver, gall bladder, stomach from right foot and small and large intestine from left foot, spinal cord, solar plexus and hypophysis from both foot. It was given once a week for 12 weeks. Dietary modification was given as per the BMI. Six women (BMI: 18.5~24.9) received 1500 kcal/day and fourteen (BMI ≥ 25) women received 1200 kcal/day. A food exchange list was given to the participants and a dietary diary was maintained to monitor the intake. The women were instructed to walk 30 minutes per day for 5 days a week. Before beginning the exercises, advised to do warm-up exercises for 10 minutes followed by brisk walking for 30 minutes and cool down after the walk. Individualized health education was given regarding metabolic syndrome components, causes and control measures including diet, exercises and regular follow up.
Group II: LI was given to group II. It include dietary modification according to BMI, moderate intensity exercises and structured health education.
Control Group: Control group did not receive any intervention and were advised to continue the routine care advised by the health care provider.
5. Data collection procedure
Data collection was done from February 28 to August 6 in 2019. Women who met the inclusion criteria were randomly assigned into three groups; MIP, LI and control group. Pretest was done. After assessment, intervention MIP was given to group 1 and LI was given to group II. Control group were advised to follow routine care advised by the health care provider. Post-test was done after 12 weeks of intervention among three groups. The primary author underwent training in reflexology before the study. We had a clear written intervention protocols which assisted in ensuring fidelity and adherence to the intervention protocol. Enactment of the intervention was assessed by weekly monitoring of the self-reported activity checklist and daily diary of diet consumed. Reminder messages were given through what's app group. The individualized health education was given by the investigator herself and clarified the doubts of participants.
6. Data analysis
Demographic variables were summarized as frequencies and percentages. Kolmogorov-Smirnov test was used to verify the normal distribution of the observed data. χ2 test used to verify the homogeneity of demographic and clinical variables. One-way ANOVA used to verify the homogeneity of dependent variables. Since repeated measures ANOVA was robust in 100% of the cases studied, independently of the manipulated conditions it was used to find out the effectiveness of the intervention on dependent variables [14]. Post hoc pairwise comparisons were done with Boneferroni' test and Tukey Honestly significant difference test (HSD). The analysis was carried out using SPSS statistics 16.0. p values smaller than .05 were considered statistically significant.
7. Ethical considerations
The approval for conducting the study was obtained from the Saveetha Medical College Hospital Human Ethics committee (Approval no: 003/02/2019/IEC/SMCH). Permission was obtained from the State Kudumbashree Mission and Community Development Society. The informed consent form was translated into regional language. Participants were contacted and explained the purpose and usefulness of the study. The confidentiality of the information and right to withdraw from the study were explained at their level of understanding in the regional language. The written consent was obtained.
RESULTS
Demographic and clinical characteristics of the participants were given in Table 1. χ2 test was carried out to find out the homogeneity of the participants. Homogeneity was observed in all characteristics except with regards to marital status, monthly income and menstruation (p < .05). Homogeneity of the outcome variables in the three groups were determined by one-way ANOVA and it was found homogenous (p < .05) (Table 2).
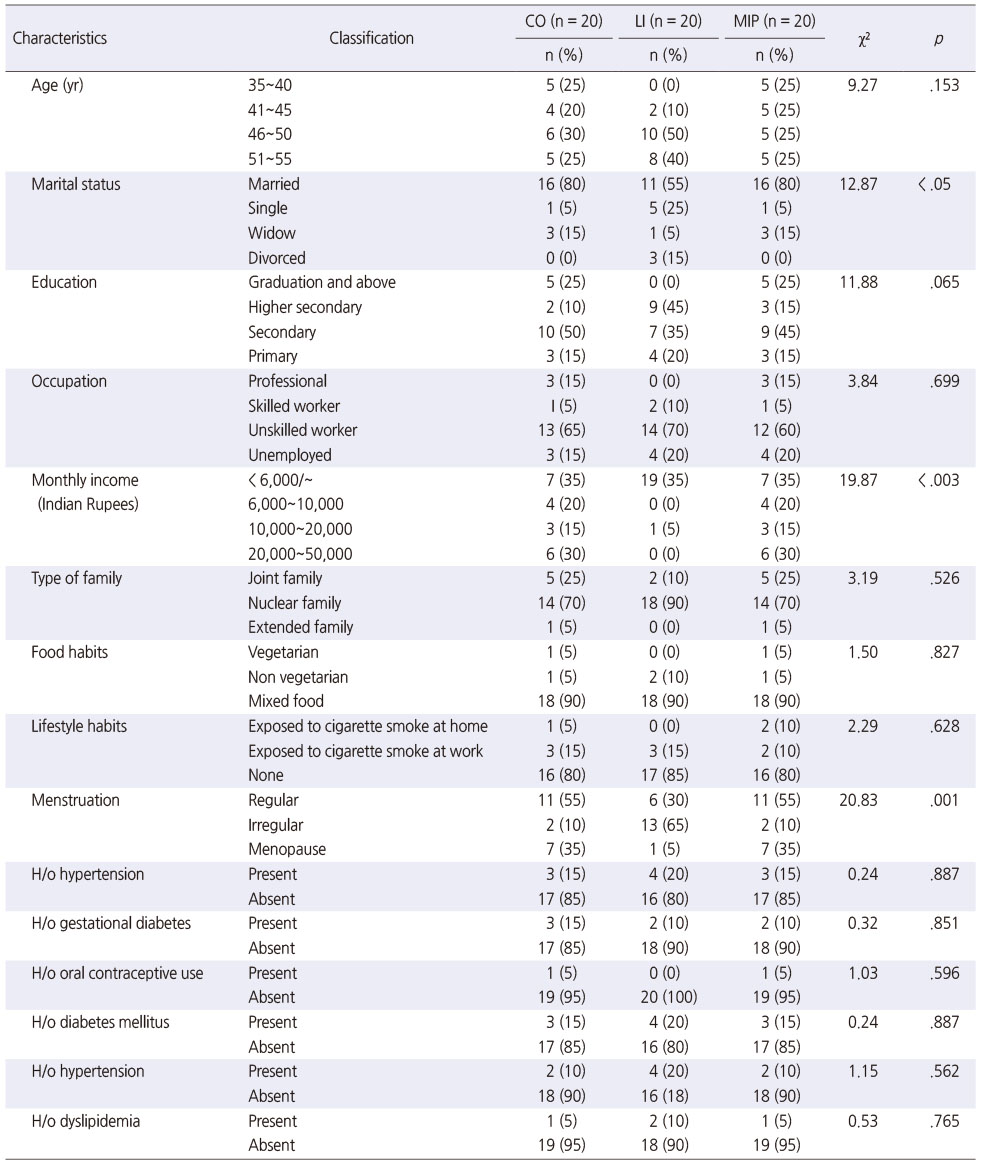
Table 1
Homogeneity Verification of General Characteristics (N = 60)
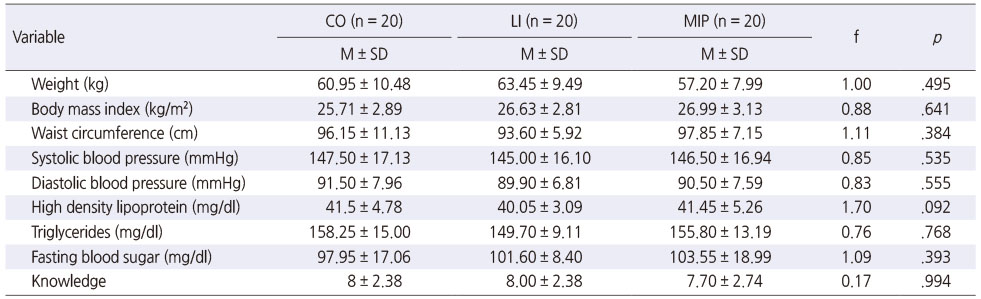
Table 2
Homogeneity Verification of Dependent Variables (N = 60)
Table 3 gives the comparison of the effectiveness of LI and MIP on physiological parameters of metabolic syndrome. The repeated measures ANOVA performed to study the effectiveness of multi interventional package on weight, BMI, waist circumference, and blood pressure. A significant difference was observed in average of all physiological parameters in MIP group and LI group compared to control group (p < .001). The mean bodyweight was decreased from 57.20 ± 7.99 kg to 51.95 ± 6.94 kg in MIP and 63.45 ± 9.49 kg to 58.40 ± 9.03 kg in LI group (p < .001), whereas, in control group it was increased from 60.95 ± 10.48 kg to 61.80 ± 11.20 kg. Similarly, BMI also reduced significantly in LI and MIP groups (p < .001) as compared to control group. The mean waist circumference in pretest of control group, LI and MIP group were 96.15 ± 11.13 cm, 93.60 ± 5.92 cm and 97.85 ± 7.15 cm respectively. The mean waist circumference in post-test of control group, LI group and MIP group were 96.00 ± 11.09 cm, 90.38 ± 6.08 cm and 93.20 ± 10.17 cm respectively. It was found to be statistically significant (p < .001) on posttest. The mean systolic BP in MIP group was decreased from 146.50 ± 16.94 mmHg to 138.40 ± 14.79 mmHg and in LI group from (145.00 ± 16.00 mmHg to 139.60 ± 13.42 mmHg), whereas, in control group BP was increased from 147.50 ± 17.13 mmHg to 149.00 ± 16.34 mmHg. The average of diastolic BP in MIP group and LI group were significantly reduced (90.50 ± 7.59 mmHg to 85.80 ± 6.55 mmHg and 89.90 ± 6.81 mmHg to 87.55 ± 6.30 mmHg respectively) as compared to control group (91.50 ± 7.96 mmHg to 91.35 ± 7.21 mmHg). Bonferroni's pairwise comparison observed a significant difference in weight between control and MIP group (p < .05). Similarly, the difference in diastolic blood pressure between control group and MIP group was also significant in posttest (p < .05). Though there was no statistically significant difference in other physiological parameters between the different groups, the observed difference was clinically significant.
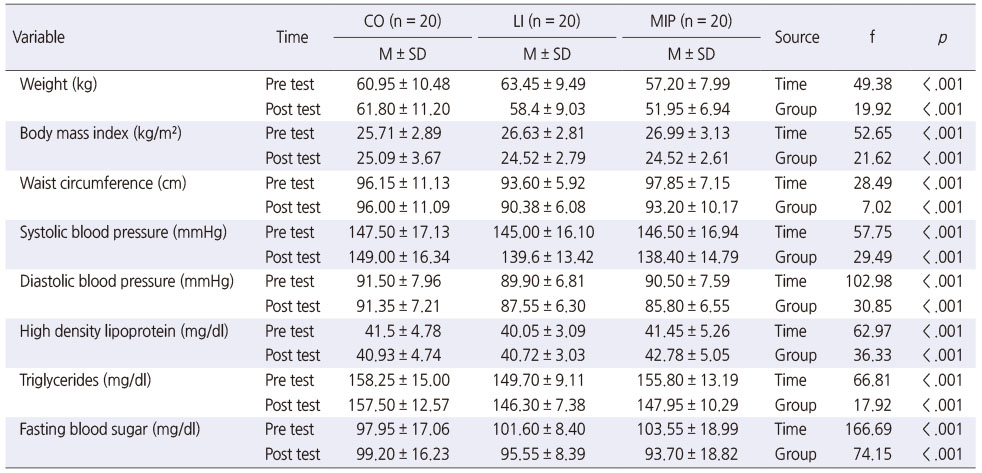
Table 3
Mean, SD and RM-ANOVA of Physiological and Biochemical Parameters among Control (CO), Lifestyle Intervention (LI) and Multi Interventional Package (MIP) Group (N = 60)
As shown in Table 3, the results of repeated measures ANOVA were significant on the level of p < .001. The results of repeated measures ANOVA indicates that there was a significant difference in the means of biochemical parameters among MIP group and LI group during pretest and post-test as compared to control group. While considering the mean HDL level, only slight improvement was noted in MIP group (41.45 ± 5.26 mg/dl to 42.78 ± 5.05 mg/dl) and LI groups (40.05 ± 3.09 mg/dl to 40.72 ± 3.03 mg/dl), but no change was found in control group. The mean triglycerides decreased from 155.80 ± 13.19 mg/dl to 147.95 ± 10.29 mg/dl in MIP group and 149.70 ± 9.11 mg/dl to 146.30 ± 7.38 mg/dl in LI group, whereas, in control group no change was observed. The mean value of FBS among MIP group reduced from 103.55 ± 18.99 mg/dl to 93.70 ± 18.82 mg/dl in MIP group and (101.60 ± 8.40 mg/dl to 95.55 ± 8.39 mg/dl) in LI group. While, an increase was observed in control group from 97.95 ± 17.06 mg/dl to 99.20 ± 16.23 mg/dl. Pairwise comparison in posttest observed a significant difference in triglycerides of control group with MIP group and LI group (p < .05).
Kruskal Wallis test was performed to study homogeneity of the socio-psychological variable. No significant difference in the mean values among control, LI and MIP group in the pretest (p = .093). The mean post-test knowledge of women in LI and MIP groups found significantly different from control (p < .001). Repeated measures ANOVA showed significant improvement in the knowledge of women in LI and MIP group (p < .001) (Table 4). But it was not significant in the control group (p = .453). Tukey HSD post hoc analysis found significant difference between MIP group and control group and between LI group and control group (p < .001). Whereas, no difference was found between LI group and MIP group.

Table 4
Mean, SD and RM-ANOVA of Knowledge among Control (CO), Lifestyle Intervention (LI) and Multi Interventional Package (MIP) Group (N = 60)
DISCUSSION
The current study aims to compare the effectiveness of multi interventional package and lifestyle interventions. This study substantiates that application of LI, and MIP had significant effect in improving the physiological, biochemical and socio-psychological variables of metabolic syndrome. Significant reduction in bodyweight, BMI and waist circumference was found among women in the MIP group and LI group compared to control group. These findings of the study are consistent with the results of a similar study among 30 obese women who had a body mass index of over 25 kg/m2 and over 30% in body fat; a nutritional intervention program every 2 weeks with a mandatory exercise intervention for 12 weeks found a significant decrease in in body weight [15]. A secondary analysis of Finnish diabetic prevention study to assess the effectiveness of LI on metabolic syndrome also had similar findings; a significant decrease in the prevalence of abdominal obesity, high blood pressure, low HDL and elevated cholesterol in the intervention group [16]. A 12-week randomized trial to find out the effect of a lifestyle education intervention alone or with partial meal replacement in obese Thai adults with metabolic syndrome found greater percentage of weight loss in lifestyle education intervention plus meal replacement compared to lifestyle education intervention alone [17]. All the above studies highlight the need for adopting dietary modifications and exercises for managing metabolic syndrome.
The current study incorporated the reflexology foot massage along with lifestyle interventions in multi interventional package. The study found a significant reduction in the systolic and diastolic BP of women among both MIP group and LI group. A similar study found a significant reduction in FBS, SBP, DBP, triglycerides and waist circumference with exercise intervention as well as reflexology intervention for 12 weeks [18]. Similarly, Saboya et al.'s study [19] on metabolic syndrome showed significant reduction in BMI, waist circumference and systolic blood pressure after 12 weeks of intervention. Another study found foot reflexology and aroma foot reflexology were effective in decreasing BP and pulse rate in essential hypertension patients [20].
In this study, we found a significant improvement in the HDL, triglycerides and FBS among women in the MIP group and LI group. A similar study also noticed that lifestyle intervention significantly reduced the prevalence of central obesity, hypertriglyceridemia and incidence of diabetes [21]. A six-month treatment with dietary modification and medium intensity walking exercises also strengthen the findings of the present study [22]. A study on short term family centered lifestyle interventions on various associated anthropometric and metabolic parameters found statistically significant improvement in BMI, systolic and diastolic BP, total cholesterol, LDL, triglycerides, PPBS and leptin levels [23]. The present study MIP group received reflexology foot massage sessions 30 minutes once in a week. Tawfik et al.'s [24] observed statistically significant decrease in lipoproteins level in the reflexology group compared to the control group. Similar study also found that foot reflexology significantly reduced the systolic and diastolic BP in hypertensive patients [10]. Similarly, in her study, Thomas [25] found that foot reflexology was effective in reducing the serum glycemic levels among the diabetic patients. These studies strongly support reflexology foot massage for controlling blood pressure and blood sugar. Therefore, these interventions can be strongly recommended to control metabolic syndrome.
There were a significant improvement in the knowledge of women in MIP group and LI group compared to control group in this study. A similar study found that consumption of fresh fruits and vegetables, dairy products, whole grain products, and steamed vegetables in the diet significantly increased and the proportion of white bread, processed meat, starchy foods and sweets significantly decreased after an education program. Significant improvement was also observed in physical activity, systolic blood pressure, waist circumference levels, high-density lipoproteins cholesterol and glucose levels [26]. In another study, guided risk management strategy was effective in terms of change in knowledge and attitude score [27]. These findings point out the need for providing knowledge on metabolic syndrome and its control measures for strict adherence to the intervention protocol.
One strength of this study is that it included three groups of women with two intervention group and one control group. Another strength of the study is that it is one of the first few studies conducted in India among middle aged self-help group women where metabolic syndrome was addressed. The intervention was provided by the trained researchers. However, one limitation of the study was the limited sample size. Hence larger studies are required with bigger sample size to generalize the findings. The self-reported activity check list and dietary diary were the source of information to ensure that participants followed the interventions. Another limitation was that subjects were perimenopausal women. Thus the results of the study cannot be generalized to all women.
CONCLUSION
The study results substantiate that 12 weeks of MIP as well as LI significantly improved the physiological, biochemical and socio- psychological parameters of metabolic syndrome among women. MIP is effective to control body weight, BMI, BP, HDL, triglycerides and FBS and to increase knowledge on MS. Considering the limitations of the study, there is a need for more comprehensive studies with large sample size to generalize the findings.
Notes
This manuscript is based on a part of the first author's doctoral dissertation from Saveetha University. Year of 2020.
CONFLICTS OF INTEREST:The authors declared no conflict of interest.
AUTHOR CONTRIBUTIONS:
Conceptualization or/and Methodology: Elizabeth AJ & Aruna S & Mercy PJ.
Data curation or/and Analysis: Elizabeth AJ.
Funding acquisition: Elizabeth AJ.
Investigation: Elizabeth AJ & Aruna S & Mercy PJ.
Project administration or/and Supervision: Elizabeth AJ & Aruna S & Mercy PJ.
Resources or/and Software: Elizabeth AJ.
Validation: Elizabeth AJ & Aruna S & Mercy PJ.
Visualization: Elizabeth AJ & Aruna S & Mercy PJ.
Writing original draft or/and Review & editing: Elizabeth AJ & Aruna S & Mercy PJ.
ACKNOWLEDGEMENTS
The authors wish to acknowledge all the women who participated in the study.
References
-
Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive summary of the Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). JAMA 2001;285(19):2486–2497. [doi: 10.1001/jama.285.19.2486]
-
-
Lanktree MB, Hegele RA. Metabolic syndrome. In: Ginsburg GS, Willard HF, editors. Genomic and Precision Medicine: Cardiovascular Disease. 3rd ed. Amsterdam: Academic Press; 2017. pp. 47-63.
-
-
Bentley-Lewis R, Koruda K, Seely EW. The metabolic syndrome in women. Nature Clinical Practice Endocrinology & Metabolism 2007;3(10):696–704. [doi: 10.1038/ncpendmet0616]
-
-
Carr MC. The emergence of the metabolic syndrome with menopause. The Journal of Clinical Endocrinology & Metabolism 2003;88(6):2404–2411. [doi: 10.1210/jc.2003-030242]
-
-
Elshamy K, Elsafety E. Effect of nursing interventions using foot reflexology on blood pressure and quality of life of hypertensive patients at Mansoura University hospitals: Preliminary results. Medical Journal of Cairo University 2011;79(2):193–202.
-
-
Martín-Timón I, Sevillano-Collantes C, Segura-Galindo A, Del Cañizo-Gómez FJ. Type 2 diabetes and cardiovascular disease: Have all risk factors the same strength? World Journal of Diabetes 2014;5(4):444–470. [doi: 10.4239/wjd.v5.i4.444]
-
-
Whitehead AL, Julious SA, Cooper CL, Campbell MJ. Estimating the sample size for a pilot randomised trial to minimise the overall trial sample size for the external pilot and main trial for a continuous outcome variable. Statistical Methods in Medical Research 2016;25(3):1057–1073. [doi: 10.1177/0962280215588241]
-
-
Blanca MJ, Alarcón R, Arnau J, Bono R, Bendayan R. Non-normal data: Is ANOVA still a valid option? Psicothema 2017;29(4):552–557. [doi: 10.7334/psicothema2016.383]
-
-
Chaiyasoot K, Sarasak R, Pheungruang B, Dawilai S, Pramyothin P, Boonyasiri A, et al. Evaluation of a 12-week lifestyle education intervention with or without partial meal replacement in Thai adults with obesity and metabolic syndrome: A randomised trial. Nutrition and Diabetes 2018;8(1):23 [doi: 10.1038/s41387-018-0034-0]
-
-
Arslan F, Güven ŞD, Özcan A, Vatansev H, Taşgin Ö. The effect of exercise, reflexology and chrome on metabolic syndrome. International Journal of Medical Research & Health Sciences 2018;7(8):77–85.
-
-
Saboya PP, Bodanese LC, Zimmermann PR, Gustavo AD, Macagnan FE, Feoli AP, et al. Lifestyle intervention on metabolic syndrome and its impact on quality of life: A randomized controlled trial. Arquivos Brasileiros de Cardiologia 2017;108(1):60–69. [doi: 10.5935/abc.20160186]
-
-
Lee HS, Kim DO. The effects of aroma foot reflexology and foot reflexology on blood pressure, pulse rate and blood lipid level of elderly essential hypertensive patients in a rural area. Journal of the Korea Academia-Industrial Cooperation Society 2012;13(9):4053–4064. [doi: 10.5762/KAIS.2012.13.9.4053]
-
-
Tawfik RM, Hassan Z, El-nahas N, Soliman A. Effect of reflexology on lipoproteins in women with type 2 diabetes mellitus. Medical Journal of Cairo University 2017;85(2):509–513.
-
-
Thomas JM. A comparative study on the effectiveness of foot reflexology on glycemic levels among diabetics with oral hypoglycemic agents and insulin therapy from a selected old age home at Mangalore. International Journal of Advanced Science and Research 2016;1(10):6–12.
-
-
Soósová MS, Hrehová J. The effect of education on lifestyle changes and metabolic syndrome components. Central European Journal of Nursing and Midwifery 2014;5(4):161–168. [doi: 10.15452/CEJNM.2014.05.0012]
-
-
Paul A, Molly J. Effectiveness of a guided risk management strategy on the knowledge and attitude regarding the prevention of metabolic syndrome among adolescents. International Journal of Community Medicine and Public Health 2016;3(6):1564–1567. [doi: 10.18203/2394-6040.ijcmph20161629]
-
 Cite
Cite
