 Submit an article
Submit an article
Articles
- Page Path
- HOME > J Korean Acad Nurs > Volume 51(5); 2021 > Article
- Research Paper Validity and Reliability of the Turkish Version of the COVID Stress Scale
- Demirgöz Bal Meltem, Dişsiz Melike, Bayri Bingöl Fadime
-
Journal of Korean Academy of Nursing 2021;51(5):525-536.
DOI: https://doi.org/10.4040/jkan.21106
Published online: October 31, 2021
1Midwifery Department, Marmara University, Health Sciences Faculty, Istanbul, Turkey
2Department of Obstetrics and Gynecology Nursing, Health Sciences University, Hamidiye Faculty of Nursing, Istanbul, Turkey
2Department of Obstetrics and Gynecology Nursing, Health Sciences University, Hamidiye Faculty of Nursing, Istanbul, Turkey
Abstract
Purpose
The aim of this study was to assess the Turkish adaptation of the COVID Stress Scale (CSS) on the basis of determining the stress caused by the coronavirus disease (COVID-19) pandemic, and to test its validity and reliability.
Methods
The English CSS was translated into Turkish using forward and backward translation. Data were collected online from 360 participants. Construct validity was evaluated using confirmatory factor analysis, exploratory factor analysis, and content validity. Pearson product-moment correlation, Cronbach’s alpha reliability coefficient, and test-retest methods were used to evaluate reliability.
Results
The Turkish version of the CSS has 36 items consistent with the original scale and has five factors: COVID danger and contamination, socioeconomic consequences of COVID, COVID xenophobia, traumatic stress due to COVID, and compulsive checking for COVID. The construct validity of the Turkish version of the CSS was verified by the adjusted goodness of fit index > .85, and comparative fit index > .95. The content validity index of each item was 91%. The corrected item-total correlations of the scale ranged from .51 to .89. Internal consistency was reliable, with a Cronbach’s α of .93.
Conclusion
The Turkish version of the CSS is valid and reliable. It can be used as a measurement tool for the assessment of COVID-related stress.
J Korean Acad Nurs. 2021 Oct;51(5):525-536. English.
Published online Oct 31, 2021.
https://doi.org/10.4040/jkan.21106
Published online Oct 31, 2021.
https://doi.org/10.4040/jkan.21106
© 2021 Korean Society of Nursing Science
Original Article
Validity and Reliability of the Turkish Version of the COVID Stress Scale
Abstract
Purpose
The aim of this study was to assess the Turkish adaptation of the COVID Stress Scale (CSS) on the basis of determining the stress caused by the coronavirus disease (COVID-19) pandemic, and to test its validity and reliability.
Methods
The English CSS was translated into Turkish using forward and backward translation. Data were collected online from 360 participants. Construct validity was evaluated using confirmatory factor analysis, exploratory factor analysis, and content validity. Pearson product-moment correlation, Cronbach's alpha reliability coefficient, and test-retest methods were used to evaluate reliability.
Results
The Turkish version of the CSS has 36 items consistent with the original scale and has five factors: COVID danger and contamination, socioeconomic consequences of COVID, COVID xenophobia, traumatic stress due to COVID, and compulsive checking for COVID. The construct validity of the Turkish version of the CSS was verified by the adjusted goodness of fit index > .85, and comparative fit index > .95. The content validity index of each item was 91%. The corrected item-total correlations of the scale ranged from .51 to .89. Internal consistency was reliable, with a Cronbach's α of .93.
Conclusion
The Turkish version of the CSS is valid and reliable. It can be used as a measurement tool for the assessment of COVID-related stress.
Keywords
Reliability and Validity; Factor Analysis; COVID-19; COVID-19 Stress Syndrome
INTRODUCTION
Pandemics that caused great and miscellaneous damage to the whole world have been encountered throughout history [1]. The last pandemic that humanity has faced is the coronavirus disease (COVID-19) pandemic. This virus, which first appeared in China (Wuhan region), spread rapidly worldwide. The situation was declared a pandemic by the World Health Organization (WHO) on March 11, 2020. Our country, Turkey, was ranked sixth in the world among countries with the most confirmed cases. There have been 6 million confirmed cases of COVID-19 with 60 thousand deaths, reported to WHO according to current data in Turkey. The number of people who have received two doses of vaccine in Turkey is only around 20 million (25% of the total population) [2].
COVID-19 is a disease with high morbidity and mortality rates [3, 4, 5]. At the same time, during the pandemic, people can experience many negative emotions, such as the risk of infection, getting sick, fear of death, feeling of helplessness, and stigma. On the other hand, lockdowns on social life, such as the closure of schools and the restrictions on transportation, have caused constant and high levels of stress [4, 5, 6].
In our country, there were many factors affecting stress levels in this situation. Inconsistent quarantine rules applied during the COVID-19 pandemic period, such as no restrictions during weekdays, lockdown during weekends, restrictions on older persons, and no restrictions on middle-aged persons. Most of these inconsistencies were due to social and economic problems. The public did not have sufficient financial resources during this quarantine period. Therefore, there were hundreds of suicides [7]. Inconsistent statements were made by politicians about the use of masks, the ways of reducing the spread of the virus, and the application of the vaccine. Due to the speculations in social media, extreme anxiety prevailed among the public. People began to experience communication problems, increased anger, irritability, depression, and anxiety. The lack of opportunities to engage in social activities outside the home, families were forced to spend more time indoors at home, which led to more tension and irritability. For all these reasons, stress and anxiety have increased in our population [7, 8].
It is known that stress and anxiety play an important role in shaping the behavioral responses of people [9]. People with too little anxiety about a viral outbreak are less likely to be hygienic, less likely to adhere to physical distance, and are less likely to get themselves vaccinated. On the other hand, people with excessive stress and anxiety can interpret mild infections as serious infections, and they may go to hospitals and clinics unnecessarily and also exhibit socially destructive behaviors [10]. Given t he role of a nxiety a nd stress in shaping our behavior, it is critical for healthcare professionals to comprehend this situation. However, it has been reported worldwide that COVID-19 anxiety and stress assessment scales are mostly one-dimensional and have limited psychometric properties [11, 12, 13]. In our country, only a short form of the Coronavirus Anxiety Scale Turkish version is available to evaluate this anxiety level. The scale is quite short, consisting of only five items [14]. A more detailed tool is needed to measure the COVID-related stress. It is predicted that this need can be met by the scale developed by Taylor et al. [11]. In this context, the aim of this study is to adapt the COVID Stress Scale (CSS), which is a comprehensive and multidimensional measurement tool, for Turkish society.
METHODS
1. Study design
This is a methodological study.
2. Setting and samples
The study population comprised students from a state university and their families. Improbable random sampling method was used to select the sample for the study. The sample consisted of 360 participants who were aged between 18 and 55 years, were able to understand and communicate in Turkish, had access to the online data form, had no physical disability for participating in the study, and agreed to participate. Since it is recommended to determine the sample size to include 5~10 people for each scale item in scale studies, the number of participants selected was 360, which was 10 times the number of scale items (36 items) [15, 16]. The study group was formed for re-testing (n = 24) and those participating in the pilot study (n = 20) were not included in this number.
3. Measurements/instruments
The data were collected online through the CSS developed by Taylor et al. [11] and adapted for Turkish language, as well as through the descriptive information form. In the Turkish version of the validity and reliability study of the CSS, the guidelines accepted as the standard in our country for validity and reliability studies in the field of nursing were used [15, 16].
1) Descriptive information form
This form, covering individual characteristics of the participants (age, education status, income level, chronic illness, etc.) are composed of a total of 13 questions.
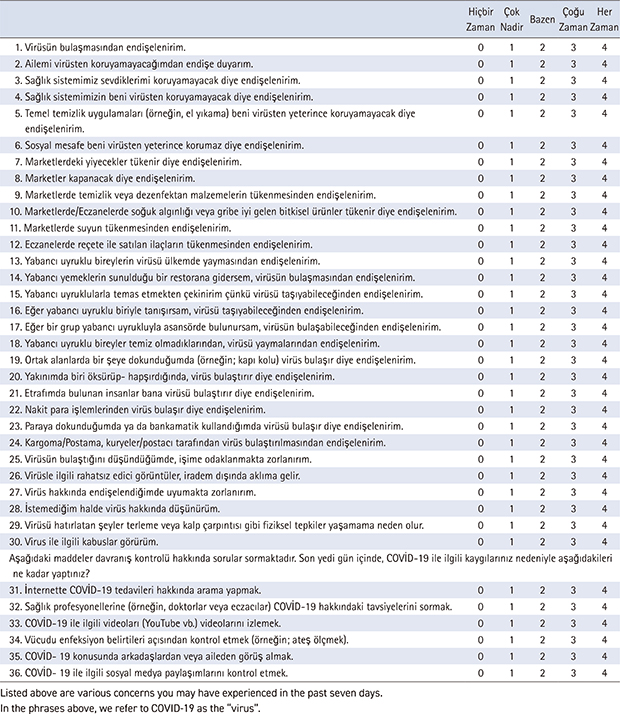
2) COVID Stress Scale
This is a self-report scale with 36 items developed by Taylor et al. [11] to evaluate the stress experienced during the COVID-19 period. Before taking up the Turkish adaptation of the scale, permission was obtained from Taylor et al. [11], who developed the scale. The scale was prepared as a five-point Likert scale to determine the severity of symptoms. The scale is composed of five subscales as in the original form: COVID danger and contamination (1, 2, 3, 4, 5, 6, 19, 20, 21, 22, 23, and 24), socioeconomic consequences of COVID (7, 8, 9, 10, 11, and 12), COVID xenophobia (13, 14, 15, 16, 17, and 18), traumatic stress due to COVID (25, 26, 27, 28, 29, and 30), and compulsive checking for COVID (31, 32, 33, 34, 35, and 36). Although there are no reverse-coded items in the scale, each item is answered by considering how the individual defines the item according to his/her experience during the COVID-19 pandemic. Participants determined how they felt and how often they experienced the feelings during the last seven days, and gave 0 points if the answer was Never, 1 point if it was Very rarely, 2 points if it was Sometimes, 3 points if it was Most of the time, and 4 points if the answer was Always. Higher mean scores indicated an increased stress level associated with the COVID-19 pandemic [11].
4. Data collection/procedure
The study was conducted from December 2020 to January 2021, on participants meeting the study criteria, using an online data collection method. The form, which took an average of 10~15 minutes to answer, was sent to the participants online (google doc. forms). All participants (n = 360) completed the form in full. The data were collected online through via google doc.
Application for permission to conduct the research was made to the Ministry of Health and permission was obtained (2020-11-12T13_31_40). Permission was also obtained from the Ethics Committee of the Faculty of Health Sciences at Marmara University (26.11.2020/69). In addition, online consent of the participants meeting the inclusion criteria was obtained by informing them about the purpose and method of the study, and it was stated that they could withdraw from the study at any time.
1) Providing language equivalence
To evaluate the content validity of the scale, the original English version of the CSS was translated into Turkish by a psychiatric nursing lecturer, a gynecological nursing lecturer, and an English lecturer [11]. The researchers reviewed the translated scale and prepared a joint Turkish text. The suitability and comprehensibility of the prepared text were evaluated by a Turkish teacher. In the next stage, the scale was translated back into English by two faculty members whose mother tongue is Turkish, who have been living in the USA for 10 years, and hold a PhD. Both faculty members did not see the original version of the scale before the translation. The scale, which was translated back into English, was translated back into Turkish by a faculty member (lecturer in psychiatric nursing and gynecological nursing). The semantic change of the original scale was evaluated, and the scale was put into the final form.
2) Content validity analysis
After completing the language validity of the scale, the Turkish version of the scale was sent to 13 experts to determine the content validity, and their opinions were obtained. To evaluate the degree of measurement of each item, they were asked to score the items between 1 and 5 (1 = totally inappropriate, 2 = inappropriate, 3 = appropriate, 4 = quite appropriate, 5 = totally appropriate). Opinion differences among experts were analyzed using Lawshe's technique, and the data obtained from the experts were evaluated using the Content validity index (CVI). The CVI of the items was determined to be 91%. As a result of the evaluations made by the experts, the scale was evaluated by applying a pilot study to 20 people who were not included in the main study, and the necessary corrections were made.
5. Data analysis
The data were analyzed using the Statistical Package for the Social Sciences (SPSS) version 21.0 and SPSS Analysis of Moment Structures (AMOS) 26.0 program (IBM Corp., Armonk, NY, USA). In the reliability analysis of the scale, Pearson's correlation coefficient was calculated using the test-retest method in the evaluation of time invariance. The Pearson product-moment correlation coefficient for the item-total correlation coefficient and Cronbach's alpha reliability coefficient for the internal consistency coefficient were calculated for the internal consistency evaluation. Lawshe's technique was used in the evaluation of expert opinions for the content validity of the scale, and exploratory factor analysis (EFA) and confirmatory factor analysis (CFA) were used to evaluate construct validity.
6. Ethical consideration
Application for permission to conduct the research was made to the Ministry of Health and permission was obtained (2020-11-12T13_31_40). Permission was also obtained from the Ethics Committee of the Faculty of Health Sciences at Marmara University (26.11.2020/69). In addition, online consent of the participants meeting the inclusion criteria was obtained by informing them about the purpose and method of the study, and it was stated that they could withdraw from the study at any time.
RESULTS
It was determined that the mean age of the participants was 28.4 ± 6.93 (min: 18, max: 55) a nd their duration of education was 15.4 ± 2.33 (5~22) years. Moreover, a great majority of the participants (86.4%) were single and unemployed (75.8%), and more than half of them (62.5%) had an income equal to their expenses. More than half of the participants (67.4%) were living in a city center, 10.6% had at least one child, 16.9% were smokers, 8.5% had chronic diseases such as asthma, hypertension, and heart disease, and 7.2% received support from a psychologist or psychiatrist during the COVID-19 pandemic.
1. Reliability analysis
1) Item analysis
The item-total score correlations of the Turkish version of the CSS are given in Table 1. When the item-total score correlations of 36 items were examined for the reliability study of the Turkish version of the CSS, it was determined that the reliability coefficient varied between .51 and .89 and the correlation between item scores and total scale scores was positive and statistically significant (p < .001) (Table 1).
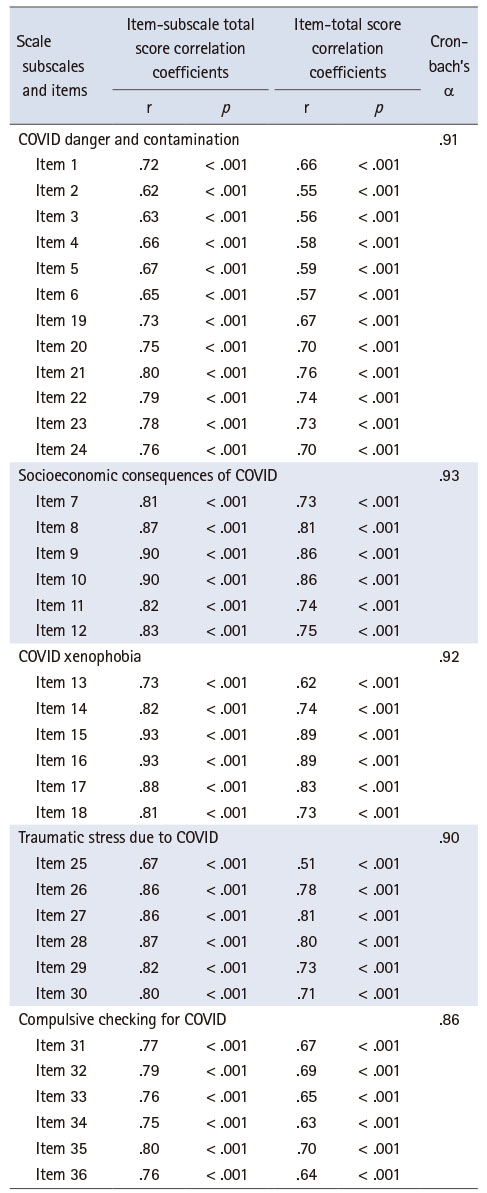
Table 1
COVID Stress Scale Subscales Item-Subscale Total Score Correlations (N = 360)
When the item-subscale total score correlations of each subscale of the Turkish version of the CSS were examined, it was determined that the reliability coefficient of the 12 items in the COVID danger and contamination subscale ranged between r = .62 and .80, the reliability coefficient of six items in the socioeconomic consequences of COVID subscale ranged between r = .81 and .90, the reliability coefficient of six items in the COVID xenophobia subscale ranged between r = .73 and .93; the reliability coefficient of six items in the traumatic stress due to COVID subscale ranged between r = .67 and .87, and the reliability coefficient of six items in the compulsive checking for COVID subscale ranged between r = .76 and .80, and the correlation coefficients of all items were positive and statistically significant (p < .001) (Table 1).
2) Reliability coefficient of internal consistency
In the analysis made for internal consistency in the reliability study of the Turkish version of the CSS, the Cronbach's alpha reliability coefficients were determined as α = .91 for the COVID danger and contamination subscale, α = .93 for the socioeconomic consequences of COVID subscale, α = .92 for the COVID xenophobia subscale; α = .90 for the traumatic stress due to COVID subscale, α = .86 for the compulsive checking for COVID subscale (Table 1), and α = .93 for the whole scale.
3) Test and retest
In testing the time-invariance of the Turkish version of the CSS, which was adapted to Turkish, test-retest measurements conducted with 24 participants with a two-week interval were evaluated with Pearson product-moment correlation and t-test. When the correlation between the scores obtained from the first and second applications of the Turkish version of the CSS and its subscales was examined with Pearson correlation analysis, the reliability coefficient between the scores of two measurements made for the scale and five subscales varied between .04 and .97, and no correlation was found between the subscales except for the total scores of the scale (Table 2). When the test-retest mean scores of the participants were compared with the independent groups t-test, no statistically significant difference was found between the mean scores (p > .05) (Table 2).
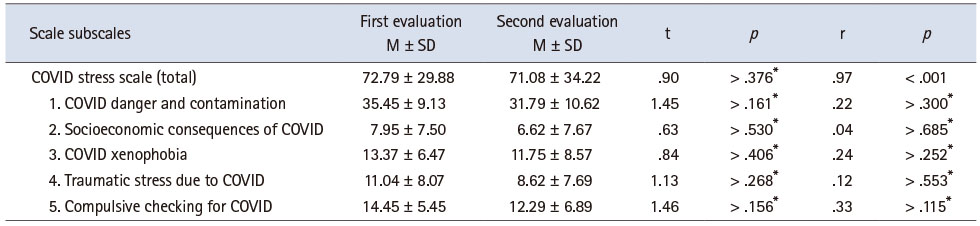
Table 2
Comparison of Test and Re-Test Mean Scores of COVID Stress Scale and Sub-Dimensions, and Correlations (N = 30)
2. Validity analysis
The language validity and content validity of the scale were determined and are stated in the data collection and procedure section.
1) Exploratory factor analysis
First, an EFA was performed to determine the construct validity of the Turkish version of the CSS. In this study, the factor analysis was performed by obtaining data as 10 times the number of items (n = 360) for the construct validity of the Turkish version of the CSS with 36 items. In addition, the Kaiser-Meyer-Olkin (KMO) test was conducted to determine the suitability of the data for factor analysis, and Bartlett's test was applied to determine the significance and zero difference between the variables to be analyzed. The KMO coefficient was found to be .83, the chi-square value for Bartlett's test (χ2 = 2749.62; df = 66; p < .001) was highly significant (p < .001), and the data were suitable and sufficient for the factor analysis. The maximum likelihood method and oblique (oblimin) rotation method were used in the factor analysis. It was found that the eigenvalue of the scale with a total of 36 items in the Turkish version of CSS and its subscales was above 1.00, with five factors accounting for 65% of the total variance (Table 3).
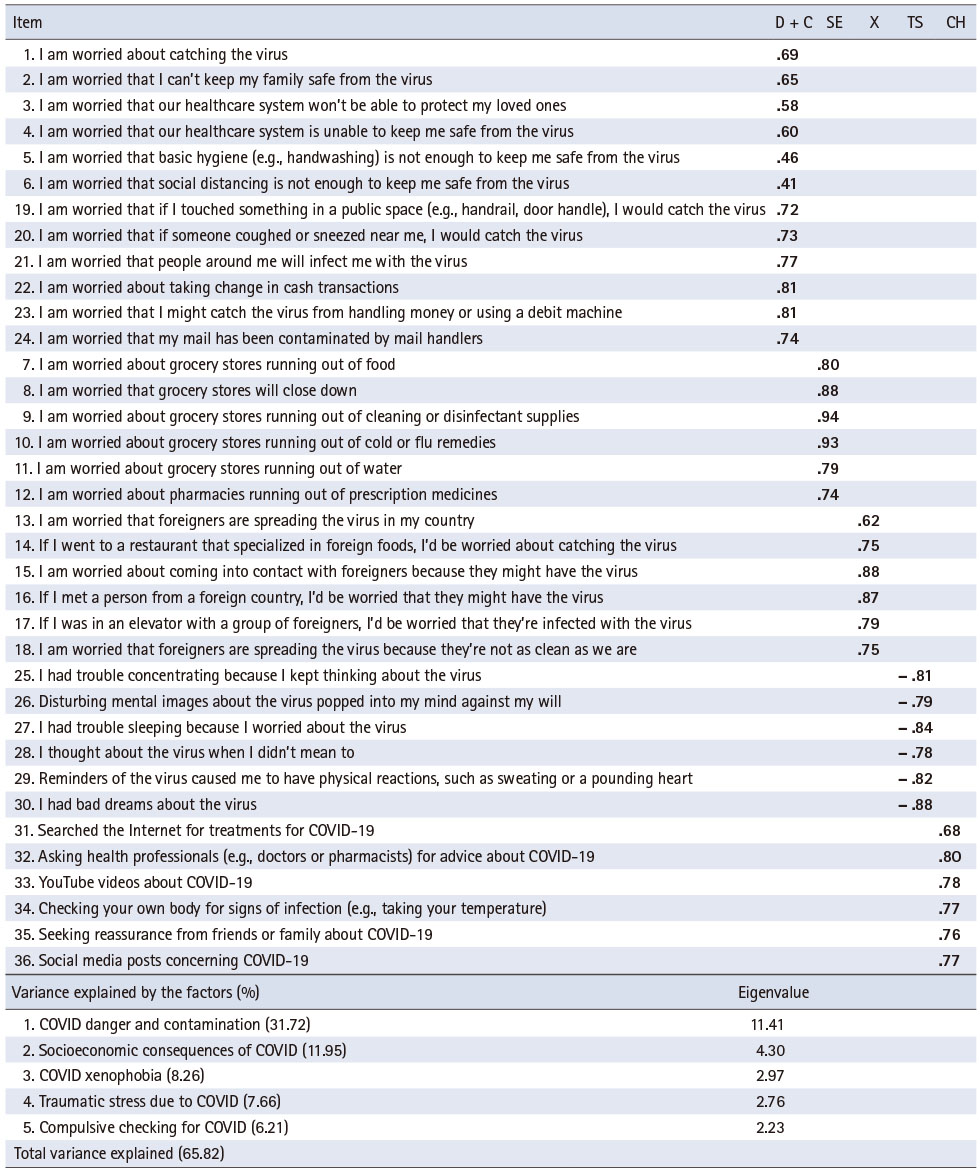
Table 3
Exploratory Factor Analysis: Factor Loadings (N = 360)
The items remained in the original and recommended form of the scale, and the factors were named as follows.
(1) COVID danger and contamination
This factor group consists of 12 items, including items 1, 2, 3, 4, 5, 6 (danger) and 19, 20, 21, 22, 23, and 24 (contamination).
(2) Socioeconomic consequences of COVID
This factor group consists of a total of six items including items 7, 8,9,10,11, and 12.
(3) COVID xenophobia
This factor group consists of six items, including items 13, 14, 15, 16, 17, and 18.
(4) Traumatic stress due to COVID
This factor group consists of six items, including items 25, 26, 27, 28, 29, and 30.
(5) Compulsive checking for COVID
This factor group consists of six items, including items 31, 32, 33, 34, and 36 (Table 3).
2) Confirmatory factor analysis
The recommended CFA standard goodness of fit index measures [17] are shown in Table 4. As a result of the five-factor CFA, the fit indices were found to be Chi-square = 546.29 (p < .001), degree of freedom = 156 (χ2 = 546.29; df = 156, χ2/df = 3.50), root mean square error of approximation (RMSEA) = .08 (p < .05) standardized root-mean-square residual (SRMR) = .04, comparative fit index (CFI) = .92, non-normed fit index (NNFI) = .95, goodness of fit index (GFI) = .95, and adjusted goodness of fit index (AGFI) = .94. The factor loads obtained as a result of the CFA of all items were determined to be between .50 and .91. Figure 1 shows a CFA diagram.
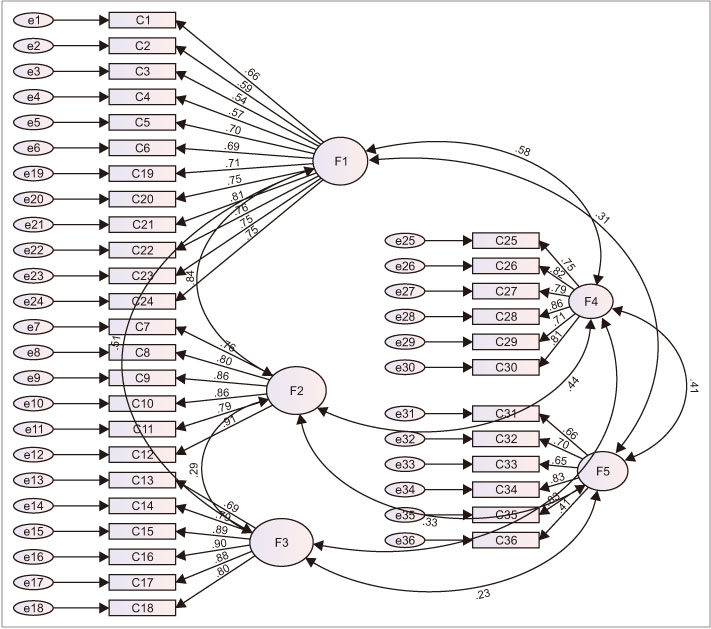
Figure 1
COVID stress scale five-factor confirmatory factor analysis diagram.
C = Item no; e = Residual covariance matrix; F1 = COVID Danger and contamination; F2 = Socioeconomic consequences of COVID; F3 = COVID xenophobia; F4 = Traumatic stress due to COVID; F5 = Compulsive checking for COVID.
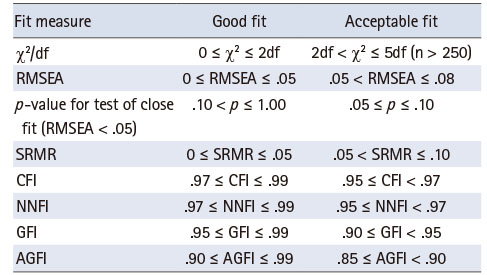
Table 4
Recommended Standard Goodness of Fit Criteria
DISCUSSION
In this study, a validity and reliability study of the CSS was conducted, and the Turkish version of the CSS was found to have good psychometric properties. There are a limited number of studies on the stress caused by COVID-19 in Turkey.
In the reliability analysis of the Turkish version of the CSS, test-retest, internal consistency, and item analysis were performed. Test-retest reliability is the power of a measurement tool to provide consistent results from application to application and to show time invariance. The test-retest correlation analysis results of the Turkish version of the CSS showed that there was no statistically significant correlation between the subscales, but there was a strong correlation for the overall scale [15, 16]. Retest reliability is recommended if the measured property has a structure that shows continuity [18]. The fact that there was no statistically significant difference between the subscales in this study showed that it was not affected by time. Another supporting result for the reliability of the scale was that the internal consistency coefficient was statistically significant. To evaluate the internal consistency of the scale, Cronbach's alpha technique, which is suitable for Likert-type scales, was used. It is assumed that the higher the alpha coefficient of the scale, the more consistent the items in the scale, and it is composed of items predicting the components of the same property. The alpha coefficient, which lies between 0 and 1 with the average of the total variances of the items with the overall variance, determines whether the questions in the scale form a whole to explain a homogeneous structure [17, 19]. In the analysis of internal consistency in the reliability study of the Turkish version of the CSS, the Cronbach's alpha reliability coefficient was determined to be at the desired level in five subscales and was highly similar to the internal consistency coefficients of the original scale [11]. The internal consistency coefficients of the subscales of the original scale, which were found to be highly reliable, were found to be between .86~.93 in this study. In addition, they were between .85 and .94, and.86 and .95 in the Canadian and the United States of America samples, respectively [11].
If the items in a scale have equal weights and are in the form of independent units, the correlation coefficient between each item and the total values is expected to be high. The higher the correlation coefficient, the higher the correlation of that item with the property to be measured [17, 19]. Although there is no specific standard regarding when the reliability will be deemed insufficient for the criterion below which the item total score correlation coefficient falls, the correlations are recommended not to be negative and to be above .25 and .30 [20]. It should be noted that the higher the correlation coefficient, the better the reliability of the items [17, 19]. It was observed in the item analysis performed for the item reliability of the Turkish version of CSS that the correlation of the subscale score of all items in the scale with the scale total score was above the value of .30, as stated in the literature. This result means that all items measured the same attitude [20].
However, a high level of agreement among experts is an important result of the content validity of the scale [21]. In conclusion, it can be asserted that the scale has an understandable language structure and content.
As a result of the EFA conducted to determine the construct validity of the Turkish adaptation of the scale, the items having factor loads of < .40, and the items that were involved in more than one factor simultaneously and had the difference between loads in two factors below 0.20, were eliminated and a scale consisting of 36 items as in the original scale was obtained. As a result of the analysis performed in accordance with the literature, a structure with an eigenvalue greater than 1 and a total variance of over 50% was obtained [22, 23]. In EFA, the adequacy of the sample is determined based on the KMO value [20]. KMO value between.90 and .99 is considered as perfect, between .80 and .89 as very good, between .70 and .79 as good, between .60 and .69 as moderate, between .50 and .59 as weak, and below .50 as unacceptable [17]. In this study, the KMO and Bartlett test results are consistent with the EFA results reported in the literature.
In the literature, the use of EFA and CFA analyses in the same sample remains controversial. It is suggested that if the sample size is adequate (> 300), both EFA and CFA analyses can be performed on the same population [24]. Consistent with the literature [14, 25], analyses were performed on the same sample used in this study. Using CFA, the representation level of the items in the determined subscale and their adequacy in explaining the structure were tested [15, 16]. For this purpose, the commonly used goodness of fit tests, chi-square fit statistics, RMSEA, SRMR, CFI, NNFI, GFI, and AGFI were used [15, 16]. The goodness of fit statistics should be at the desired level in the CFA [15, 16]. On the other hand, the fit indices of the 5-item short form of the Coronavirus Anxiety Scale, which was studied in Turkey, are RMSEA = .09, GFI = .98, AGFI = .94, CFI = .98, and NNFI = .97, which were determined to be within acceptable values. This was in agreement with the results of a previous study [14]. The results of the study indicated that all goodness of fit values of the scale adapted χ2/df, SRMR, RMSEA, GFI, AGFI, NNFI, and CFI were above the acceptable limit values. From a holistic framework, the results obtained showed that the adapted model is acceptable.
It is very important to detect symptoms and intervene early before any psychopathology develops in individuals. The Turkish version of the CSS is a valid and reliable measurement tool for assessing the COVID-19 stress scale. It can be a valuable tool for assessing the stress caused by the pandemic (Appendix 1).
However, the Turkish version of the CSS is not aimed at establishing a diagnosis of stress disorder. It should not be ignored that the scale has the function of referring to psychotherapist/psychiatrist experts only in accordance with the obtained scores. Since all data collected for the stress levels caused by COVID-19 are based on personal statements, the error margin should be taken into account. In addition, the data were not collected face-to-face. Individuals with psychopathologies were not identified. There could be a possibility of bias in the answers, and of reliability problems. Furthermore, older individuals with lower socioeconomic levels could not be reached during the online data collection process.
CONCLUSION
The results of the study showed that the Turkish version of the CSS had sufficient validity and reliability. The internal consistency and validity values were compatible with the values obtained in the original study. Therefore, it can be asserted that the scale has sufficient psychometric properties to evaluate the stress associated with the COVID-19 pandemic. In line with these results, the use of the Turkish version of CSS in determining the stress level for the COVID-19 pandemic can be recommended by considering that it is easy, understandable, and can be filled quickly.
Researchers should focus on the effect of COVID-19 on the vulnerable population living in rural areas and on the lower socioeconomic strata, who face barriers in accessing health care. There is a need to develop mental health interventions that health professionals can use effectively.
Notes
CONFLICTS OF INTEREST:The authors declared no conflict of interest.
AUTHOR CONTRIBUTIONS:
Conceptualization or/and Methodology: Demirgöz Bal M & Dişsiz M & Bayri Bingöl F.
Data curation or/and Analysis: Dişsiz M.
Funding acquisition: None.
Investigation: Demirgöz Bal M & Dişsiz M.
Project administration or/and Supervision: Demirgöz Bal M& Dişsiz M.
Resources or/and Software: Dişsiz M.
Validation: Demirgöz Bal M & Dişsiz M.
Visualization: Demirgöz Bal M & Dişsiz M & Bayri Bingöl F.
Writing original draft or/and Review & Editing: Demirgöz Bal M & Dişsiz M.
ACKNOWLEDGEMENTS
We would like to thank all the participants and the experts who shared their valuable opinions.
DATA SHARING STATEMENT
Please contact the corresponding author for data availability.
Appendix 1
COVID Stress Scale
References
-
Huremović D. Brief history of pandemics (pandemics throughout history). In: Huremović D, editor. Psychiatry of Pandemics: A Mental Health Response to Infection Outbreak. Cham, Switzerland: Springer; 2019. pp. 7-35.
-
-
World Health Organization (WHO). WHO coronavirus (COVID-19) dashboard [Internet]. Geneva: WHO; c2021 [cited 2021 Jul 17].Available from: https://covid19.who.int/ .
-
-
Gamonal-Limcaoco S, Montero-Mateos E, Lozano-López MT, Maciá-Casas A, Matías-Fernández J, Roncero C. Perceived stress in different countries at the beginning of the coronavirus pandemic. International Journal of Psychiatry in Medicine. 2021 Jul 16;Forthcoming.
-
-
Wang C, Pan R, Wan X, Tan Y, Xu L, Ho CS, et al. Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID-19) epidemic among the general population in China. International Journal of Environmental Research and Public Health 2020;17(5):1729 [doi: 10.3390/ijerph17051729]
-
-
Özdin S, Bayrak Özdin Ş. Levels and predictors of anxiety, depression and health anxiety during COVID-19 pandemic in Turkish society: The importance of gender. International Journal of Social Psychiatry 2020;66(5):504–511. [doi: 10.1177/0020764020927051]
-
-
Shi L, Lu ZA, Que JY, Huang XL, Liu L, Ran MS, et al. Prevalence of and risk factors associated with mental health symptoms among the general population in China during the coronavirus disease 2019 pandemic. JAMA Network Open 2020;3(7):e2014053 [doi: 10.1001/jamanetworkopen.2020.14053]
-
-
Yuan S, Liao Z, Huang H, Jiang B, Zhang X, Wang Y, et al. Comparison of the indicators of psychological stress in the population of Hubei province and non-endemic provinces in China during two weeks during the coronavirus disease 2019 (COVID-19) outbreak in February 2020. Medical Science Monitor 2020;26:e923767 [doi: 10.12659/MSM.923767]
-
-
Biçer I, Çakmak C, Demir H, Kurt ME. [Coronavirus anxiety scale short form: Turkish validity and reliability study]. Anadolu Kliniği 2020;25 Suppl 1:216–225. [doi: 10.21673/anadoluklin.731092]Turkish.
-
-
Çakir Ç, Aydin Güngör T. Cultural Competence Scale (CCS): The study of adaptation to Turkish, validity and reliability. International Journal of Contemporary Educational Studies 2016;2(1):24–36.
-
-
Çapık C, Gözüm S, Aksayan S. [Intercultural scale adaptation stages, language and culture adaptation: Updated guideline]. Florence Nightingale Journal of Nursing 2018;26(3):199–210. [doi: 10.26650/FNJN397481]Turkish.
-
-
Ozdamar K. In: [Structural equation modelling for scale and test development]. Eskişehir: Nisan Pub; 2016. pp. 45-59.Turkish.
-
-
Hair JF Jr, Gabriel MLDS, da Silva D, Braga Junior S. Development and validation of attitudes measurement scales: Fundamental and practical aspects. RAUSP Management Journal 2019;54(4):490–507. [doi: 10.1108/RAUSP-05-2019-0098]
-
-
Moretti EA, Anholon R, Rampasso IS, Silva D, Santa-Eulalia LA, Ignácio PSA. Main difficulties during RFID implementation: An exploratory factor analysis approach. Technology Analysis and Strategic Management 2019;31(8):943–956. [doi: 10.1080/09537325.2019.1575351]
-
-
Büyüköztürk Ş. In: [Handbook of data analysis for social sciences]. Ankara: Pegem Academy Pub; 2016. pp. 34-43.Turkish.
-
-
Arafat SMY, Chowdhury HR, Qusar MMAS, Hafez MA. Cross-cultural adaptation & psychometric validation of research instruments: A methodological review. Journal of Behavioral Health 2016;5(3):129–136.
-
-
Kline RB. In: Principles and practice of structural equation modeling. 4th ed. New York (NY): The Guilford Press; 2016. pp. 41-71.
-
-
Ullman JB, Bentler PM. Structural equation modeling. In: Weiner I, Schinka JA, Velicer WF, editors. Handbook of Psychology. 2nd ed. Hoboken (NJ): John Wiley & Sons, Inc.; 2012. pp. 661-690.
-
-
Artan T, Meydan S, Irmak HS. Turkish version of the fear of COVID-19 scale: Validity and reliability study. Archives of Health Science and Research 2021;8(2):117–123. [doi: 10.5152/ArcHealthSciRes.2021.20113]
-
 Cite
Cite
