 Submit an article
Submit an article
Articles
- Page Path
- HOME > J Korean Acad Nurs > Volume 52(5); 2022 > Article
- Research Paper Moderating the Effects of Health Behaviors on Sexual Intercourse among Adolescents: A CrossSectional Study Using the 2020 Adolescent Health Behavior Survey
- Eunmi Lee, Youngran Yang
-
Journal of Korean Academy of Nursing 2022;52(5):499-510.
DOI: https://doi.org/10.4040/jkan.22080
Published online: October 31, 2022
1College of Nursing, Jeonbuk National University, Jeonju, Korea
2College of Nursing · Research Institute of Nursing Science, Jeonbuk National University, Jeonju, Korea
2College of Nursing · Research Institute of Nursing Science, Jeonbuk National University, Jeonju, Korea
Abstract
Purpose
This study investigated the association between adolescent health behaviors (drinking, smoking, and drug use) and sexual intercourse, as well as the moderating effects of economic status, cohabitation with parents, and school type, among adolescents in Korea.
Methods
Secondary data from the 16th Adolescent Health Behavior Survey (2020) were used. A total of 395 schools and 54,948 middle and high school students participated in the study. Complex sample frequency analysis, the Rao–Scott test, and complex sample logistic regression analyses were performed.
Results
Sexual intercourse rates for men and women were 5.8% and 3.3%, respectively. Approximately 7.3% of high school students and 1.8% of middle school students reported having had sexual relations. Drinking (odds ratio [OR] = 3.15, 95% confidence interval [CI] = 2.82~3.52), smoking (OR = 6.75, 95% CI = 5.90~7.71), and drug use (OR = 3.03, 95% CI = 2.23~4.11) significantly increased the risk of sexual intercourse. Economic status and school type had moderating effects on the association between drinking and sexual intercourse.
Conclusion
Adolescent drinking, smoking, and drug use are associated with a higher risk of sexual experience. Thus, to reduce this risk, controlling alcohol consumption, smoking, and drug use is necessary. In addition, programs for healthy lifestyles and sexual intercourse should be differentiated according to the school type and the economic conditions of the adolescents’ households.
J Korean Acad Nurs. 2022 Oct;52(5):499-510. English.
Published online Oct 31, 2022.
https://doi.org/10.4040/jkan.22080
Published online Oct 31, 2022.
https://doi.org/10.4040/jkan.22080
© 2022 Korean Society of Nursing Science
Original Article
Moderating the Effects of Health Behaviors on Sexual Intercourse among Adolescents: A Cross-Sectional Study Using the 2020 Adolescent Health Behavior Survey
Eunmi Lee ,1
and Youngran Yang2
,1
and Youngran Yang2
Abstract
Purpose
This study investigated the association between adolescent health behaviors (drinking, smoking, and drug use) and sexual intercourse, as well as the moderating effects of economic status, cohabitation with parents, and school type, among adolescents in Korea.
Methods
Secondary data from the 16th Adolescent Health Behavior Survey (2020) were used. A total of 395 schools and 54,948 middle and high school students participated in the study. Complex sample frequency analysis, the Rao–Scott test, and complex sample logistic regression analyses were performed.
Results
Sexual intercourse rates for men and women were 5.8% and 3.3%, respectively. Approximately 7.3% of high school students and 1.8% of middle school students reported having had sexual relations. Drinking (odds ratio [OR] = 3.15, 95% confidence interval [CI] = 2.82~3.52), smoking (OR = 6.75, 95% CI = 5.90~7.71), and drug use (OR = 3.03, 95% CI = 2.23~4.11) significantly increased the risk of sexual intercourse. Economic status and school type had moderating effects on the association between drinking and sexual intercourse.
Conclusion
Adolescent drinking, smoking, and drug use are associated with a higher risk of sexual experience. Thus, to reduce this risk, controlling alcohol consumption, smoking, and drug use is necessary. In addition, programs for healthy lifestyles and sexual intercourse should be differentiated according to the school type and the economic conditions of the adolescents’ households.
Keywords
Adolescent; Sexual Intercourse; Health Behavior
INTRODUCTION
Sexual curiosity surges in adolescence because of physical changes in secondary sexual characteristics and an increase in sex hormones. The longing to feel new emotions through romantic love or to attempt physical contact to achieve sensual desire also increases during this period [1]. Consequently, the longer gender norms are not clearly established, the more likely it is that adolescents engage in impulsive sexual intercourse [2].
Sexual intercourse during adolescence exposes individuals to physical risks such as unplanned pregnancy and sexually transmitted diseases (STDs) [3]. For example, 21 million pregnancies were reported among adolescent girls aged 15 to 19 years in developing countries in 2016; nearly half (49%) were unintentional (43% in Asia, 45% in Africa, and 74% in Latin America and the Caribbean) [4]. In 2020, 410,000 young people (aged 10~24 y) were newly infected with HIV [5]
Sex during adolescence can also be associated with engagement in risky behaviors such as substance use, violence, and risky sexual practices, which are common during this period and cause significant public health concerns. Sexual behavior acquired in adolescence has been reported to be a predictor of substance use and antisocial behavior [6], risky sexual behavior (e.g., having multiple sex partners), and adverse health outcomes (e.g., STDs, unintended pregnancy) in adulthood [7].
Underage sex appears to be more prevalent in Asian countries. For example, in Thailand, 17.9% of adolescents had experienced sexual experiences, and 12.9% had sex before the age of 15 years in 2016 [8]. Male and female adolescents aged 15 to 17 years had sexual experience, respectively, in Shanghai (2.8%, 2.1%), Taipei (13.4%, 10.2%), and Hanoi (0.4%, 0.1%) [9]. In South Korea, 5.9% of middle and high school students stated that they had sexual experiences [10]. This percentage has continued to increase over the years.
Sexual experiences during adolescence may lead to sexual intercourse as a result of engaging in deviant or antisocial behaviors [6]. Various antecedent factors, such as drinking, smoking, and drug use, act in complex ways [6, 11]. According to previous studies, the risk of sexual experiences was 2.95 to 3.04 times higher in adolescents who drank regularly than in those who did not [12, 13]. The number of respondents who said they drank before sexual intercourse was high (33.6%~51%), and the majority reported engaging in risky sex without contraception [14, 15]. The rate of sexual experience was significantly higher among adolescents who responded that they smoked [11, 16, 17] or used drugs [6, 11]. The state induced by alcohol and drugs cannot be judged as a level of complete consciousness; thus, special management is required to recognize alcohol and drug use as a risk factor that may lead to misinterpreting another person’s sexual expression or unwanted sexual intercourse [18, 19].
During adolescence, young people are influenced by their surrounding environment and learn to interact and develop relationships [20]. Thus, from an ecological perspective, a multifaceted approach that includes the impact of socio-environmental contexts is necessary [21, 22]. For example, adolescents are influenced by how their friends react to sex [23, 24]. Having friends of the opposite sex [25] or no close friends of the same sex [26] can also significantly affect their sexual experience. Adolescents’ sexual behavior is also influenced by family characteristics; for example, individuals who live with both parents have a higher likelihood of practicing sexual abstinence and protective sexual behavior [27]. Being separated from parents for personal and situational reasons, acquiring sexual information through the behavior of family members, and the family’s economic level are factors reported to produce different results on sexual experience [26, 28, 29, 30]. One’s educational environment also influences adolescents’ sexual behaviors; for instance, public school students were more likely to have sexual intercourse with and without condom use (odds ratio [OR] = 1.72 and 1.69, respectively) than to abstain from sexual intercourse [31]. Some studies have examined the moderating effects of sexual behavior in adolescents. For example, peer acceptance of early sex predicts more risky sexual behavior. On the one hand, this was only true for adolescents whose mothers engaged in high levels of psychological control; in addition, it was true only for girls, suggesting that maternal psychological control moderated the association between peer attitudes and sexual experience [32]. On the other hand, the relationship between parental overprotection and sexual experience is stronger for male than for female adolescents and is moderated by gender [33]. Most previous studies have focused on the risk and influencing factors of adolescent sexual experience [24, 25, 26], and some have analyzed mediating effects [34]. The results showed that controlled consumption strategies moderated the effects of alcohol consumption on risky sexual behaviors [32].
Considering the complexity of understanding adolescent behavior, the effects of unhealthy behaviors among adolescents, such as drinking, smoking, and drug use, on sexual experience may differ depending on family characteristics or school type [26, 27, 28, 31]. Alcohol consumption, smoking, and drug use are impacted by family and school characteristics, which in turn affect sexual experience [35, 36, 37, 38]. However, only a few studies [35, 38] on the moderating effect of adolescent behaviors have derived additional meaningful results from the study of adolescent sexual experience. Therefore, this study investigated the effects of adolescent health behaviors (drinking, smoking, and drug use) on sexual intercourse and analyzed whether the family’s economic status, cohabitation with parents, and school type moderated the effects.
The results of this study can inform school-based adolescent sexual health education programs to promote sexual health among adolescents. In addition, it can help control unhealthy behaviors to prevent the risk of sexual experiences by developing tailored programs according to family characteristics and school types.
METHODS
1. Theoretical framework
The social-ecological model considers five levels of human development and health behaviors: intrapersonal (e.g., attitudes), interpersonal (e.g., family, peers), institutional (i.e., organizations), community (e.g., neighborhood, culture), and policy [21, 22]. The model has been widely used in research to understand adolescent sexuality in the ecological context of individuals, peers, families, parents, schools, and communities [39, 40]. Based on the social-ecological model, in this study, adolescents’ intrapersonal characteristics included gender, age, academic performance, alcohol consumption, smoking, and drug use. The interpersonal characteristics of the home environment factors included parental education level, economic level, and residence status (whether they were living with parents). Finally, school type was included as an institutional influence.
2. Study design
This secondary data analysis employed the 16th Adolescent Health Behavior Survey (2020), which was conducted directly by the Ministry of Education, the Ministry of Health and Welfare, and the Korea Centers for Disease Control and Prevention (KCDC) (approval number:117058).
3. Study data and participants
Data from the 16th Adolescent Health Behavior Survey (2020) were used in accordance with the regulations on disclosure procedures for raw data from the KCDC. The Adolescent Health Behavior Survey is an anonymous, self-reported online survey distributed to middle and high school students in Korea to identify health behaviors such as smoking, drinking, obesity, eating habits, and physical activity.
Data from middle and high schools nationwide (as of April 2019) were used in the sampling design of the 16th Adolescent Health Behavior Survey (2020). Stratified cluster random sampling was utilized for sampling; the primary and the secondary sampling units were a school and a class, respectively. For the primary extraction, a sample school was selected using permanent random number sampling for each layer. For secondary extraction, one class was randomly selected from each grade of the selected sample school. A nationwide survey was conducted with 57,925 students from 800 schools (400 middle and 400 high schools). Due to the COVID-19 outbreak, the teachers tasked with investigation support were overburdened with work, and computer labs were unavailable. This reduced the total number of schools to 793 (398 middle and 395 high schools). Therefore, only 54,948 students participated (participation rate = 94.9%) in the study.
4. Variable measurements
1) Sexual intercourse
Sexual intercourse was measured via the answer to the question, “Have you ever had sex?” to which participants could respond either “yes” or “no.”
2) Drinking, smoking, and drug use
Drinking was classified as “yes” if the participant had drunk more than one alcoholic beverage in the previous 30 days and “no” if they had never consumed alcohol or had not drunk more than one alcoholic beverage in the past 30 days. Smoking was classified as “yes” if participants smoked even one cigarette in the last 30 days or multiple days in a month and as “no” if they had never smoked before or had smoked only one cigarette in the last 30 days. Cigarettes included all types of cigarettes, for example, liquid e-cigarettes and vapor e-cigarettes. Lastly, for drug use behavior, the raw data were used as they included the “no” and “yes” responses to the question, “Are there any drugs or substances that you have habitually used so far, aside from those for therapeutic purposes?”
3) Participant characteristics
Based on Kim et al.’s previous study [41], the participants were asked to provide their gender, school type, father’s education level, mother’s education level, and academic performance. Gender was divided into “man” and “woman,” and school type was divided into “middle school” and “high school.” Based on Pyo et al.’s previous study [42], the education levels of the fathers and the mothers were reclassified as “high school graduate or lower,” “university graduate or higher,” “other (don’t know, none),” and “refusal to respond.” For academic performance, “high” and “high-middle” were reclassified as “high,” “low-middle,” and “low” as possible responses to the question, “How has your academic performance been in the last 12 months?”
Family and school characteristics, economic status, residence status (living with or without parents), and school type were also considered. Based on previous studies, economic status was dichotomized [43]; “high,” “high-middle,” and “middle” were reclassified as “high,” and “low-middle” and “low” were reclassified as “low” in response to the question of “What is the economic status of your household?” The question on “Cohabitation with parent/s” asked if participants were currently living with at least one of their parents. The school types were divided into “coed,” “all-girls,” and “all-boys.”
5. Data analysis
The Adolescent Health Behavior Survey used a complex sampling design method. Therefore, we followed the data analysis guidelines for the complex sample design of the KCDC. The complex sample design elements were the strata, cluster, weight (W), and finite population correction factor. The detailed statistical analysis method is as follows:
First, unweighted frequencies and weighted percentages were calculated through complex sample frequency analysis to identify individual, family, and school characteristics and health behaviors. Second, the Rao–Scott test was conducted using a cross-sample cross-analysis to identify differences in sexual intercourse according to individual, family, and school characteristics and health behaviors. Third, a complex-sample logistic regression analysis was performed to understand the moderating effect of family and school characteristics on the effects of adolescent health behaviors on sexual intercourse. The moderation effect was analyzed with logistic regression using interaction terms (e.g., drinking × economic status, smoking × school type, drug use × cohabitation with parents). Interactions are specified in the logistic regression as below, including coefficients for the predictors (drinking and economic status) and the response regarding sexual experience. If the interaction coefficient β3 is significant, the association between X and the probability that Y = 1 depends on the values of Z indicates a moderating effect [44].
Y = α + β1X + β2Z + β3XZ
Both IBM SPSS statistics 27.0 (IBM Corp., Armonk, NY, USA) and EasyFlow Statistics macro [45] were used for the data analysis, and the significance level was set at 5%.
6. Ethical considerations
The need for an Institutional Review Board (IRB) review was waived by the Jeonbuk National University IRB committee (No. IRB FILE 2022-03-007).
RESULTS
1. Participant characteristics and sexual intercourse
In total, 54,948 students participated in the 2020 survey (man: 51.9%, woman: 48.1%). Approximately 49.6% were in middle school, and 50.4% were in high school. Regarding the father’s education level, 42.9% had the highest level of education with a college degree or higher. Likewise, 41.8% of the mothers had a college degree or higher. However, 22.3% of the respondents refused to answer questions about their family members. Regarding academic performance, 67.0% and 33.0% reported high and low grades, respectively. Approximately 87.4% reported having a high economic status, whereas 12.6% stated that it was low. In addition, 76.3% lived with their parents, and 1.4% did not. Regarding school type, the majority attended coed institutions (66.5%), followed by all-boys schools (17.3%) and all-girls schools (16.2%). In terms of health behaviors, 10.7% engaged in habitual drinking, 4.8% smoked, and 0.8% habitually used drugs (excluding those for therapeutic purposes). In total, 4.6% of the adolescents had sexual experiences (see Table 1).
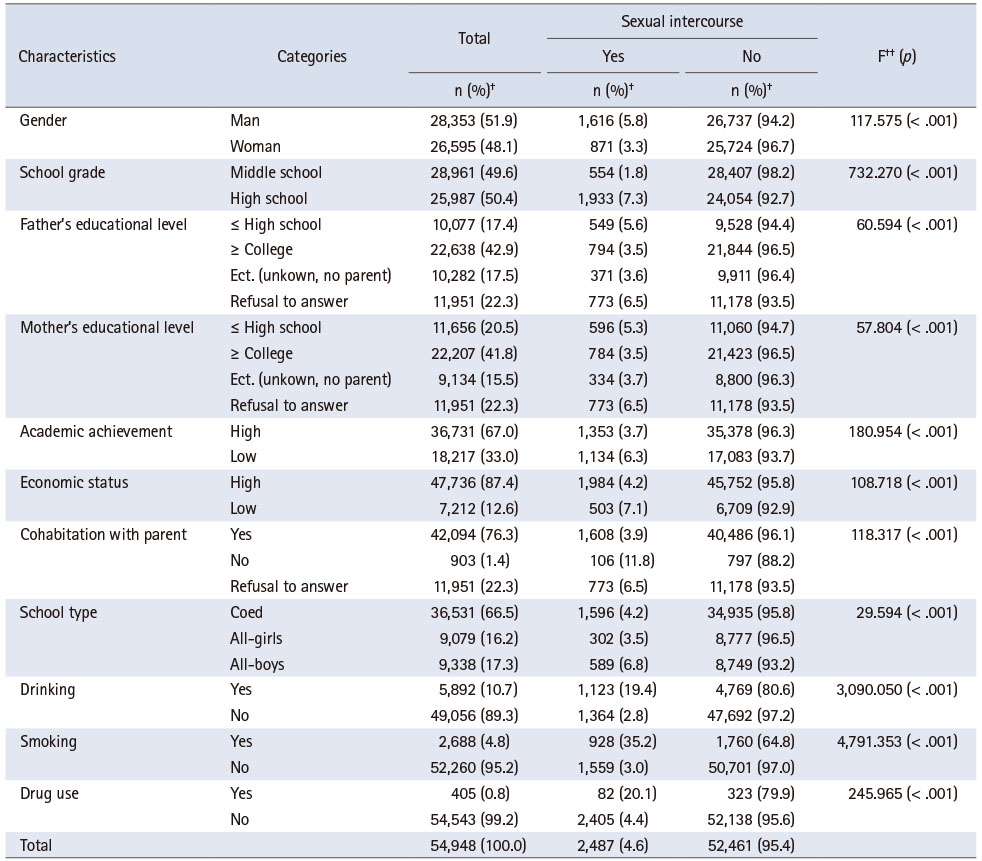
Table 1
The differences of sexual intercourse by characteristics (N = 54,948)
2. Differences in sexual intercourse according to participants’ characteristics and health behaviors
The sexual intercourse rate was 5.8% for male adolescents, which was higher than their female counterparts (3.3%). It was 7.3% for high-school students, which was higher than that for middle-school students (1.8%). The rate of sexual experience was relatively high when the father had a lower than high-school educational level or when the participant refused to respond. Similar results were found for mothers’ education levels. Those with low-intermediate academic achievement accounted for 6.3%, compared to those with intermediate-high grades or higher (3.7%). The rate of sexual experience was higher in those with the economic status of middle or lower (7.1%) than in those with a middle or high income (4.2%). The rate was 11.8% for those who did not live with their parents, which was significantly higher than that for those who lived with their parents (3.9%).
The sexual experience rate for students in all-boys schools was 6.8%, which was relatively higher than those attending all-girls (3.5%) and coed (4.2%) schools. The sexual experience rate of adolescents who habitually drank alcohol was 19.4%, which was very high compared with that of non-drinkers (2.8%). The sexual intercourse rate for those who habitually smoked was 35.2%, significantly higher compared to that of non-smokers (3.0%). The sexual intercourse rate of adolescents who habitually used drugs was 20.1%, significantly higher than that of non-drug users (4.4%) (see Table 1).
3. Main and moderating effects
Table 2 presents the main (Models 1 and 2) and moderating (Model 3) effects. Model 1 was statistically significant for gender, school grade, drinking, smoking, and drug use. The explanatory power of the model was 19.6% (McFadden R2 = 0.196). The risk of sexual experience was 1.41 times higher among male than female adolescents (95% confidence interval [CI] = 1.27~1.57) and 2.69 times higher among high school students than among middle school students (95% CI = 2.40~3.01). It was 3.18 times higher among habitual drinkers (95% CI = 2.84~3.56) than among non-drinkers, and habitual smokers were 6.77 times (95% CI = 5.93~7.74) more likely to have sexual experience than non-smokers. Meanwhile, the habitual drug users’ sexual intercourse rate was 3.24 times (95% CI = 2.40~4.36) higher than that of non-drug users.
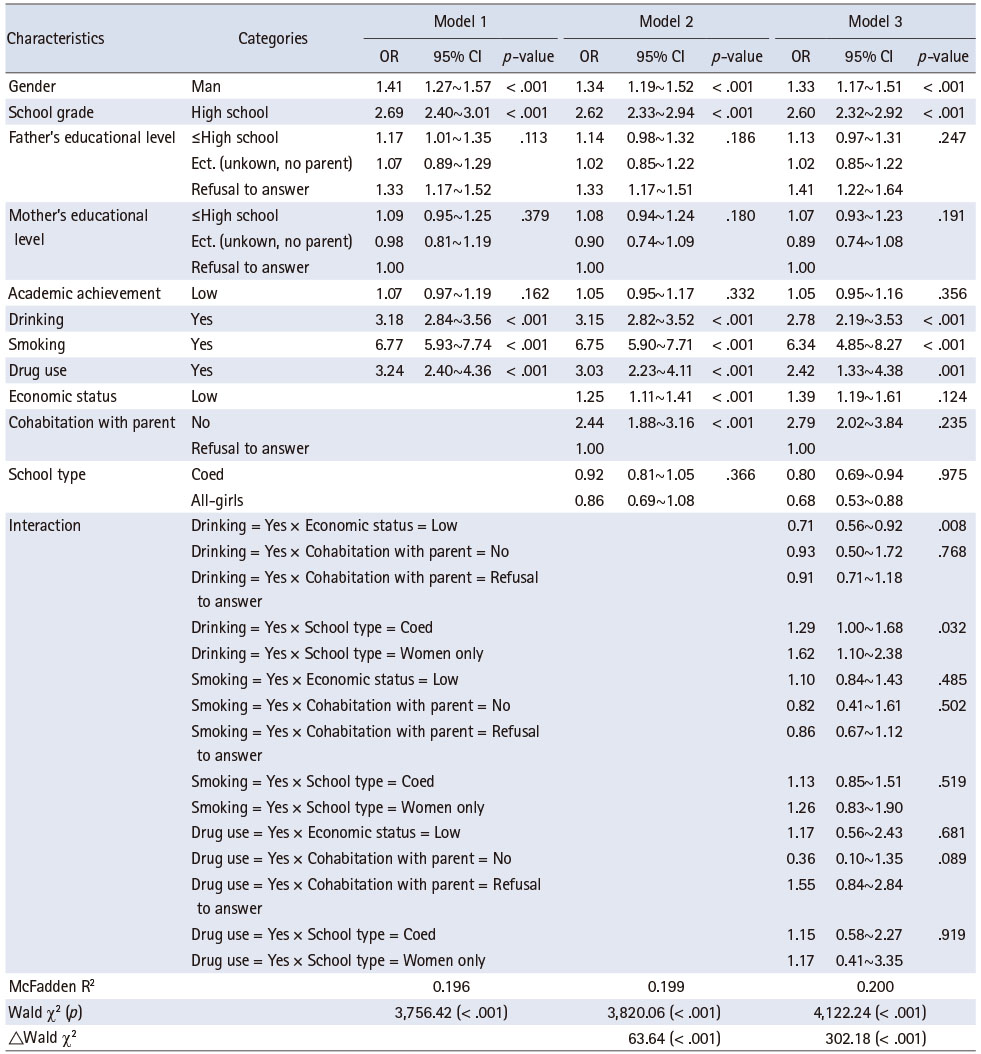
Table 2
Logistic regression model of sexual intercourse (N = 54,948)
In Model 2, the control variables of family and school characteristics were added and found to be statistically significant in terms of gender, academic grade, drinking, smoking, drug use, economic status, and cohabitation with parents. The explanatory power of the model was 19.9% (McFadden R2 = 0.199), which increased significantly by 0.3% compared with Model 1 (ΔWald χ2 = 63.64, p < .001). The risk of sexual experience was 1.25 times (95% CI = 1.11~1.41) higher for those with a low-intermediate economic status than for those with intermediate-high grades or high economic status. Moreover, it was 2.44 times higher among students who did not live with their parents or refused to respond than when at least one of their parents lived with them (95% CI = 1.88~3.16). However, school type was not significant.
Model 3 shows the results of the examination of the moderating effects of economic status, cohabitation with parents, and school type on the association between drinking, smoking, drug use, and sexual intercourse. This was found to be statistically significant for the following interaction terms: drinking and school type. The explanatory power of the model was 20.0% (McFadden R2 = 0.200), demonstrating a significant 0.1% increase compared with that of Model 2 (ΔWald χ2 = 302.18, p < .001). The risk of sexual experience was 0.71 times lower when habitual drinking was combined with low economic status (95% CI = 0.56~0.92). For students of co-educational institutions and all-girls schools who drank habitually, the risk of sexual experience was 1.29 times and 1.62 times higher than that of the students attending all-boys schools, respectively (95% CI = 1.00~1.68, 95% CI = 1.10~2.38).
DISCUSSION
Based on the ecological theory, this study investigated the effects of adolescent health behaviors (drinking, smoking, and drug use) on sexual intercourse using data from the 16th Adolescent Health Behavior Survey (2020). In addition, whether the family’s economic status, living with parents, and school type moderated these effects was also examined.
In this study, the sexual experience rate was 4.6%, which is lower than the 2019 study (5.9%), differing from the findings of the studies in Costa Rica (18.1%) and Russia (21.7%) [3, 46], likely due to differences in socio-cultural norms and environments between countries and adolescents’ varying open-mindedness regarding sexual experiences. The lower sexual experience rate compared to the previous year’s research could also be due to having fewer opportunities to contact those of the opposite sex. However, it remains unknown whether the rate dropped because of the COVID-19 pandemic or improved consciousness through high-quality sex education. Subsequently, this remains a topic for future research.
The results for the first model’s sex experience rate were significantly higher when male students attended high school and habitually drank, smoked or used drugs. According to previous studies on gender, male adolescents have a high rate of sexual experience [9, 42]. Likewise, in this study, male students had a greater sexual experience than female students. This is possibly the result of reflecting the differences in perceptions of gender norms [47], namely that male students have higher acceptance of and openness to sexual desires than female students. High school students had more sexual experience than middle school students, which reflects the results of previous studies [3, 25] that found higher sexual experience due to the increase in influences of peer groups and network utilization as age increases. Measuring the levels of seeking sexual sensation, interest in sex, and pornography consumption would help establish a healthy attitude toward sex by providing health education customized to adolescents’ gender and age.
In this study, habitual drinking was found to be a factor that increased the sexual experience rate by 3.18 times, confirming the results of prior studies [11, 17, 46] that drinking significantly increases the sexual experience of adolescents by 1.21 to 11.3 times. In addition, smoking and drug use in this study increased the sexual experience rate 6.77 times and 3.24 times, respectively, which is in line with the findings of previous studies [12, 13, 48]. Health teachers can reduce the risk of sexual experiences for students by periodically monitoring the latter’s drinking, smoking, and drug use, identifying cases of addiction and referring them to specialized institutions such as addiction prevention centers.
The adolescent participants’ drinking and smoking habits strongly correlated with their current family members’ drinking and smoking habits. If there are alcohol consumers among family members, the risk of drinking increases 6.23 times, and in the case of smokers, the smoking rate of adolescents increases 5.07 times [18]. Therefore, family members should be aware that children can imitate and learn their behavior. Likewise, communities and schools should provide periodic education to prevent adolescents from engaging in prohibited behaviors at home. In addition, to minimize the negative effects of individuals who are sensitive to friend/peer group influences [23, 24], communities and schools should form connections, both in and out of school. In particular, academies and study cafes, where adolescents are frequently concentrated, can display posters that realistically express the negative effects of drinking, smoking, and substance abuse on adolescence, which can be confirmed through social networking service (SNS) links. Guaranteed telephone services, not restricted by time and space and real-time counseling using SNS will be a practical alternative to minimize the negative impacts of adolescence.
Additionally, in Model 2, the risk of sexual experience was 2.44 times higher when adolescents did not live with their parents or refused to respond compared to when at least one parent lived with them. This is in line with Wijayanti et al.’s findings [49], which show that if parents fail to play a sound role with a preventive attitude toward their children's sexual behavior, the risk of sexual behavior increases by 2.87 times. Moreover, a study [29] in the same context showed that changes in family dynamics due to divorce or bereavement have a significant effect on adolescents’ sexual experiences. However, there was no statistically significant difference in the final model, to which additional interaction terms for family and school characteristics were added. Previous studies have found that the risk rate of sexual experience can be significantly reduced when parents monitor their children’s daily lives while significantly controlling their activities [31] and communicating openly about sex while forming intimate bonds with their children [26, 29]. Therefore, in this study, we considered that significant results were not derived from the final model because they could not reflect the qualitative factors of these interactions but only the structure of the family, thus, highlighting the need for in-depth qualitative studies in the future.
In Model 2, sexual experience was found to be 1.25 times higher for those with low to medium economic levels, which is consistent with the findings of previous studies [30, 48] that sexual experience increases as income level decreases. Families with stable financial structures have more opportunities to provide quality education to their children [43]; therefore, the risk of sexual experience is presumed to be relatively low. To combat sexual health disadvantages in adolescents arising from a family’s economic vulnerability, it is necessary to assess the family's financial situation, parent-child communication, and parents’ monitoring of their children, thereby, providing appropriate education and counseling for adolescents.
The results for the final model showed that it had a moderating influence on the combined effect of low economic status and habitual drinking. The influence of drinking on adolescents from families with good economic conditions was greater compared to the same on those from low-income families. Therefore, it is necessary to consider the differences in drinking and sexual experiences according to household income levels to reduce the risk factors for adolescent sexual experiences. Most previous studies analyzed only the risk rate of sexual experience according to economic level and did not study the moderating effect of drinking; therefore, there are limitations in a direct comparative analysis. In future studies, it will be necessary to analyze the factors of parents' monitoring level according to income level or how to change the sexual autonomy and self-esteem of adolescents according to their economic level.
The results for the final model showed that it had a moderating effect on the influence of the sexual experience of those who habitually drink alcohol among students at all-girls schools and was 1.62 times higher than that of the students at all-boys schools. This is in line with a study of a 12-month follow-up of sexual experiences showing that the sexual experience rate increases in female students (2.54 times) and male students (1.91 times) under the age of 16 years when they drink alcohol excessively [12]. In addition, in the case of frequent alcohol consumption, the risk of sexual experience of male students increased 2.2 times, while that of female students increased 3.1 times [16]. A study investigating alcohol consumption showed that the risk of sexual experience increased by 2.81 times and 7.27 times in male and female students, respectively [15]. In another study, 52.4% of female students who had sexual experiences reported drinking before sexual intercourse, and 9.5% reported that they always drank alcohol [25]. In particular, female students who blacked out due to excessive drinking had a 5.33 times higher risk of unsafe and unplanned sexual behavior and a 3.62 times higher response rate for regretting sexual activity [18], and 35.2% of women who experienced early sexual experiences between the ages of 15 and 17 said they had consumed alcohol [48]. Similarly, drinking significantly affects not only early sexual experiences but also risky sexual relationships without contraception, thereby, increasing the risk of pregnancy and STDs. In the case of women, it has been reported that when they drank alcohol, they had a lower ability to express their desire to cease engagement in sexual activity; hence, they could be more easily exposed to the risk of impulsive sexual activity. The unique classification system of middle and high schools in Korea, which classifies girls and boys by sex, made it possible to efficiently reflect meaningful interactions between the same sexes in the research results. This further proves that girls who habitually drink are more vulnerable to the negative effects of drinking than boys. Therefore, efforts must be made to introduce sex-differentiated alcohol consumption and sex education programs.
Study strengths, limitations, and future research
The first strength of this study is the use of data from the Adolescent Health Behavior Survey, which can represent Korean adolescents on sensitive topics such as sexual intercourse. The second is modeling according to the ecology theory, reflecting individual, family, and school influences, and the last one is understanding the moderating effects to provide evidence for health behavior interventions that can be more specialized for student groups, for example, by school type or student economic status. However, the study has limitations; for example, it is not possible to control for various variables that can impact adolescent sexual experience (e.g., pornography use, peer influence, parental monitoring), which should be researched in future. The use of condoms during sex and the total number of sex partners can also be added to the survey as risk factors for sexual behavior that highly affect STD infection and teen pregnancies. Multi-level analysis can be used to investigate the combined influence of individual and community characteristics on the sexual behavior of adolescents. Health Outcome and Determinants of Community is an open resource database integrated with statistics from 69 national institutes, including physical, environmental, cultural, social, and demographic characteristics that affect the health of the community (https://chs.kdca.go.kr/chs/recsRoom/dataBaseMain.do). It is possible to investigate the community-related factors of adolescents’ sexual behavior through multi-level analysis using community-level variables in this database, such as the number of major crimes per 1,000 people, the number of pubs, the number of establishments selling tobacco, and the ratio of male to female household heads.
CONCLUSION
This study was conducted to investigate the association between adolescent health behaviors (drinking, smoking, and drug use) and sexual intercourse and the moderating effects of economic status, cohabitation with parents, and school type among adolescents in Korea.
Adolescents’ unhealthy behaviors, drinking, smoking, and drug use were found to be associated with a high percentage of sexual intercourse, and the effect was moderated by economic level and school type in the association between drinking and sexual intercourse. Therefore, to efficiently reduce the risk of sexual experiences, programs catered for adolescents should focus on healthy lifestyle interventions. In addition, for those who habitually drink, customized sex education should be provided according to the school type and economic status. In the future, we suggest repeating the study on the moderating effect of habitual drinking behavior on female and male students while targeting coed schools to generalize the results. Vivid experiences and dynamics can be understood through qualitative research on the effects of drinking on sexual experiences in coed and all-girls schools.
Notes
CONFLICTS OF INTEREST:The authors declared that no conflict of interest.
AUTHOR CONTRIBUTIONS:
Conceptualization or/and Methodology: Yang Y & Lee E.
Data curation or/and Analysis: Yang Y.
Funding acquisition: Yang Y.
Investigation: Yang Y & Lee E.
Project administration or/and Supervision: Yang Y.
Resources or/and Software: Yang Y.
Validation: Yang Y & Lee E.
Visualization: NA.
Writing original draft or/and Review & Editing: Yang Y.
ACKNOWLEDGEMENTS
This study was supported by the Ministry of Education of the Republic of Korea and the National Research Foundation of Korea (NRF-2020S1A5A2A03047080).
DATA SHARING STATEMENT
Data in this study were from the 2020 Adolescent Health Behavior Survey from the Korea Centers for Disease Control and Prevention (KCDC), Ministry for Health and Welfare, Republic of Korea.
References
-
Bukenya JN, Nakafeero M, Ssekamatte T, Isabirye N, Guwatudde D, Fawzi WW. Sexual behaviours among adolescents in a rural setting in eastern Uganda: A cross-sectional study. Tropical Medicine & International Health 2020;25(1):81–88. [doi: 10.1111/tmi.13329]
-
-
World Health Organization (WHO). Reducing early and unintended pregnancies among adolescents [Internet]. Geneva: WHO; 2017 [cited 2022 Feb 7].Available from: https://apps.who.int/iris/bitstream/handle/10665/255862/WHO-
RHR- 17.10- eng.pdf.
-
-
United Nations Children’s Fund (UNICEF). HIV and AIDS in adolescents [Internet]. New York: UNICEF; 2021 [cited 2022 Oct 27].Available from: https://data.unicef.org/topic/hiv-
aids/.
-
-
Prendergast LE, Toumbourou JW, McMorris BJ, Catalano RF. Outcomes of early adolescent sexual behavior in Australia: Longitudinal findings in young adulthood. Journal of Adolescent Health 2019;64(4):516–522. [doi: 10.1016/j.jadohealth.2018.10.006]
-
-
Korea Disease Control and Prevention Agency (KDCA). Report of 2019 Adolescent Health Behavior Survey [Internet]. Cheongju: KDCA; 2019 [cited 2022 Feb 9].Available from: https://www.kdca.go.kr/yhs/home.jsp.
-
-
Furlanetto MF, Ghedin DM, Gonçalves TR, Marin AH. Individual and contextual factors associated with sexual initiation among adolescents. Psicologia: Reflexão e Critica 2019;32(1):25 [doi: 10.1186/s41155-019-0138-z]
-
-
Rios-Zertuche D, Cuchilla J, Zúñiga-Brenes P, Hernández B, Jara P, Mokdad AH, et al. Alcohol abuse and other factors associated with risky sexual behaviors among adolescent students from the poorest areas in Costa Rica. International Journal of Public Health 2017;62(2):271–282. [doi: 10.1007/s00038-016-0859-z]
-
-
Kaltiala-Heino R, Fröjd S, Marttunen M. Depression, conduct disorder, smoking and alcohol use as predictors of sexual activity in middle adolescence: A longitudinal study. Health Psychology and Behavioral Medicine 2015;3(1):25–39. [doi: 10.1080/21642850.2014.996887]
-
-
Mohanan P, Swain S, Sanah N, Sharma V, Ghosh D. A study on the prevalence of alcohol consumption, tobacco use and sexual behaviour among adolescents in urban areas of the Udupi District, Karnataka, India. Sultan Qaboos University Medical Journal 2014;14(1):e104–e112. [doi: 10.12816/0003343]
-
-
Braun-Lewensohn O, Idan O, Lindström B, Margalit M. Salutogenesis and the sense of coherence during the adolescent years. In: Mittelmark MB, Bauer GF, Vaandrager L, Pelikan JM, Sagy S, Eriksson M, et al., editors. The Handbook of Salutogenesis. Cham: Springer; 2022. pp. 139-150.
-
-
Bronfenbrenner U. Toward an experimental ecology of human development. American Psychologist 1977;32(7):513–531. [doi: 10.1037/0003-066X.32.7.513]
-
-
Muchimba M. Social-ecological predictors of risky sexual behavior among young adults. Journal of Social, Behavioral, & Health Sciences 2019;13(1):1–14. [doi: 10.5590/JSBHS.2019.13.1.01]
-
-
Settheekul S, Fongkaew W, Viseskul N, Boonchieng W, Voss JG. Factors influencing sexual risk behaviors among adolescents: A community-based participatory study. Nursing & Health Sciences 2019;21(2):186–197. [doi: 10.1111/nhs.12580]
-
-
Agudile EP, Okechukwu CA, Subramanian SV, Langer A, Geller AC. Young adult sexual behavior in South Africa: How important is parental social support? African Journal of Reproductive Health 2020;24(1):35–52. [doi: 10.29063/ajrh2020/v24i1.5]
-
-
Oliveira-Campos M, Nunes ML, Madeira FC, Santos MG, Bregmann SR, Malta DC, et al. Sexual behavior among Brazilian adolescents, National Adolescent School-based Health Survey (PeNSE 2012). Revista Brasileira de Epidemiologia 2014;17 Suppl 1:116–130. [doi: 10.1590/1809-4503201400050010]
-
-
Riggs NR, Tate EB, Ridenour TA, Reynolds MD, Zhai ZW, Vanyukov MM, et al. Longitudinal associations from neurobehavioral disinhibition to adolescent risky sexual behavior in boys: Direct and mediated effects through moderate alcohol consumption. Journal of Adolescent Health 2013;53(4):465–470. [doi: 10.1016/j.jadohealth.2013.05.017]
-
-
Ahmadi K, Khodadadi Sangdeh J, Aminimanesh S, Mollazamani A, Khanzade M. The role of parental monitoring and affiliation with deviant peers in adolescents’ sexual risk taking: Toward an interactional model. International Journal of High Risk Behaviors and Addiction 2013;2(1):22–27. [doi: 10.5812/ijhrba.8554]
-
-
Leech TG. Everything’s better in moderation: Young women’s gender role attitudes and risky sexual behavior. Journal of Adolescent Health 2010;46(5):437–443. [doi: 10.1016/j.jadohealth.2009.10.012]
-
-
Rizvi F, Williams J, Maheen H, Hoban E. Using social ecological theory to identify factors associated with risky sexual behavior in Cambodian adolescent girls and young women aged 10 to 24 years: A systematic review. Asia Pacific Journal of Public Health 2020;32(2-3):71–80. [doi: 10.1177/1010539520911493]
-
-
Kim Y, Choi S, Chun C, Park S, Khang YH, Oh K. Data resource profile: The Korea Youth Risk Behavior Web-based Survey (KYRBS). International Journal of Epidemiology 2016;45(4):1076–1076e. [doi: 10.1093/ije/dyw070]
-
-
Pyo E, An J, Jeong J, Yi Y. Effects of drinking, smoking and drug use experience on adolescents’ sexual intercourse: Using the data of the Korea Youth Risk Behavior Web-based Survey from 2010 to 2014. Journal of the Korean Society of School Health 2016;29(3):299–309. [doi: 10.15434/kssh.2016.29.3.299]
-
-
Robinson CD, Tomek S, Schumacker RE. Tests of moderation effects: Difference in simple slopes versus the interaction term. Multiple Linear Regression Viewpoints 2013;39(1):16–24.
-
-
Lee IH. EasyFlow Statistics macro [Internet]. [Iksan]: StatEdu; 2020 [cited 2022 Feb 7].Available from: https://doi.org/10.22934/StatEdu.2020.01.
-
-
Bolshakova M, Galimov A, Unger JB, Rohrbach LA, Sussman S. Russian adolescent sexual behaviour and contraceptive knowledge. Sex Education-Sexuality, Society and Learning 2020;20(5):568–582. [doi: 10.1080/14681811.2019.1705780]
-
-
Turi E, Merga BT, Fekadu G, Abajobir AA. Why too soon? Early initiation of sexual intercourse among adolescent females in Ethiopia: Evidence from 2016 Ethiopian Demographic and Health Survey. International Journal of Women’s Health 2020;12:269–275. [doi: 10.2147/IJWH.S244621]
-
-
Wijayanti YT, Martini, Prasetyowati, Fairus M. Religiosity, the role of teen parents and the exposure of pornography media to adolescent sexual behavior in East Lampung region high school. Enfermería Clínica 2020;30 Suppl 5:122–128. [doi: 10.1016/j.enfcli.2019.11.037]
-
 Cite
Cite
