 Submit an article
Submit an article
Articles
- Page Path
- HOME > J Korean Acad Nurs > Volume 53(4); 2023 > Article
- Research Paper Effects of a Modified Six-Sigma-Methodology-Based Training Program on Core Competencies in Rehabilitation Nurse Specialists
- Jiayi Gu, Lan Luo, Chengjuan Li, Sumin Ma, Fanghua Gong
-
Journal of Korean Academy of Nursing 2023;53(4):412-425.
DOI: https://doi.org/10.4040/jkan.22122
Published online: August 31, 2023
1Department of Rehabilitation, Hunan Provincial People’s Hospital (The First Affiliated Hospital of Hunan Normal University), Changsha, China
2School of Nursing, University of South China, Hengyang, China
3Department of Nursing, Hunan Provincial People’s Hospital (The First Affiliated Hospital of Hunan Normal University), Changsha, China
2School of Nursing, University of South China, Hengyang, China
3Department of Nursing, Hunan Provincial People’s Hospital (The First Affiliated Hospital of Hunan Normal University), Changsha, China
-
Corresponding author:
Fanghua Gong,
Email: 543753397@qq.com
Abstract
Purpose
Nurses play an important role in ensuring patient rehabilitation and are involved in all aspects of multidimensional rehabilitation.
Therefore, strengthening rehabilitation nursing education is vital to ascertain high-quality rehabilitation and optimum outcomes. This study examined the effectiveness of a new teaching reform—a modified Six-Sigma-based training program—against a conventional educational program on rehabilitation specialist nurses’ core competencies, post-training performance, and satisfaction.
Methods
A quasi-randomized controlled trial was conducted to assess the effectiveness of the modified training program. We recruited 56 learners from the 2020 training course at the Hunan Rehabilitation Specialist Nurse Training Base as the control group. Sixty learners from the base’s 2021 training course were recruited as the intervention group. Data were collected in a consistent manner from both groups after the training program was implemented.
Results
Those who underwent the modified training program showed better improvement in all core competencies than those who underwent the conventional training program (p < .05); the scores for theoretical knowledge, clinical nursing lectures, reviews, and nursing case management improved significantly following the teaching reform (p < 0.05). Further, overall satisfaction as well as base management and theoretical teaching satisfaction improved significantly (p < .05).
Conclusion
The modified training program strengthens rehabilitation nurses’ base management abilities; enhances their core competencies; expands their interest in and breadth, depth, and practicability of theoretical courses; and updates the teaching methods.
J Korean Acad Nurs. 2023 Aug;53(4):412-425. English.
Published online Aug 31, 2023.
https://doi.org/10.4040/jkan.22122
Published online Aug 31, 2023.
https://doi.org/10.4040/jkan.22122
© 2023 Korean Society of Nursing Science
Original Article
Effects of a Modified Six-Sigma-Methodology-Based Training Program on Core Competencies in Rehabilitation Nurse Specialists
Abstract
Purpose
Nurses play an important role in ensuring patient rehabilitation and are involved in all aspects of multidimensional rehabilitation. Therefore, strengthening rehabilitation nursing education is vital to ascertain high-quality rehabilitation and optimum outcomes. This study examined the effectiveness of a new teaching reform—a modified Six-Sigma-based training program—against a conventional educational program on rehabilitation specialist nurses’ core competencies, post-training performance, and satisfaction.
Methods
A quasi-randomized controlled trial was conducted to assess the effectiveness of the modified training program. We recruited 56 learners from the 2020 training course at the Hunan Rehabilitation Specialist Nurse Training Base as the control group. Sixty learners from the base’s 2021 training course were recruited as the intervention group. Data were collected in a consistent manner from both groups after the training program was implemented.
Results
Those who underwent the modified training program showed better improvement in all core competencies than those who underwent the conventional training program (p < .05); the scores for theoretical knowledge, clinical nursing lectures, reviews, and nursing case management improved significantly following the teaching reform (p < 0.05). Further, overall satisfaction as well as base management and theoretical teaching satisfaction improved significantly (p < .05).
Conclusion
The modified training program strengthens rehabilitation nurses’ base management abilities; enhances their core competencies; expands their interest in and breadth, depth, and practicability of theoretical courses; and updates the teaching methods.
Keywords
Educational Reform; Rehabilitation Nursing; Nurse Specialists; Education, Nursing
INTRODUCTION
1. Backgroud
Given Chinese patients’ growing demand for medical treatment, cultivating high-quality rehabilitation specialist nurses is a major task of the China Nursing Career Development Plan (2016~2020) [1], which is of great significance in developing specialist nurse teams and improving the quality of specialist nursing. Rehabilitation nurses play an important role in reducing functional impairment, promoting functional recovery, reducing complications, improving patients’ quality of life, and enabling them to return to society as soon as possible [2]. However, currently, there remains a shortage of rehabilitation nurses in many developing countries and poor areas of the world [3]. In China specifically, the existing rehabilitation nurses lack systematic knowledge and skills in rehabilitation specialties, thus not meeting the patients’ rehabilitation needs [4, 5]. Therefore, improving nurses’ rehabilitation skills is an urgent task.
Rehabilitation nursing is a well-developed specialty in many countries. However, rehabilitation nurses’ training in developing countries and some distressed areas, including China, is still in the exploratory stage [6, 7, 8], and many grassroots hospitals in China have not yet established rehabilitation medicine departments or are currently in the preparatory phase [9]. The Rehabilitation Nursing Committee of the Chinese Society of Rehabilitation Medicine was the first to start a nationwide training course for rehabilitation specialist nurses in 2013, in which recruited nurses worked for more than three years in rehabilitation departments [10]. This course required learners to finish four weeks of theory and six weeks of clinical practice training. In their training model, the committee also pioneered a specialist nurse recertification system that compels learners to place more emphasis on further specialist studies after a short period of training. Learners must pass reassessment and certification after two years to obtain a “Rehabilitation Specialist Nurse Certificate.” Further, since 2012, training courses for rehabilitation nurses have been held in various provinces and cities in China [11, 12]. However, most training courses that include basic rehabilitation nurse training emphasize skill proficiency over educational skills, critical thinking, academic development, and leadership [13]. The Rehabilitation Specialist Nurse Training Base in Hunan, China, has recruited rehabilitation specialist nurses nationwide since 2015. To promote the widespread adoption of rehabilitation nursing across all regions, the screening criteria for admission into rehabilitation specialist education programs in China are kept relatively low [14]. Due to the fact that some hospitals in remote areas of China have not yet established rehabilitation departments many learners who participated in the Hunan Provincial Rehabilitation Specialist Nurse Training Course of China in 2019 came from neurology, neurosurgery, respiratory medicine, orthopedics, and other related departments. Nurses from different departments have different knowledge reserves in rehabilitation nursing and there are also significant differences in the rehabilitation content of patients with functional impairments among different departments, which has led to an uneven reserve level of professional knowledge and different learner training needs. This has led to great difficulties in specialized teaching [15], as the conventional training method does not always meet the needs of rehabilitation specialist nurses or lead to an improvement in their core competencies, in turn, leading to diminished satisfaction with training among learners [16].
The American Association of Rehabilitation Nurses [17] states that rehabilitation specialist nurses’ core competencies are their ability to promote healthy living, provide nursing intervention, ensure interprofessional nursing, and exhibit leadership skills. The International Council of Nurses defines core competencies as personal attributes, including knowledge, skills, and attitudes [18]. A study [19] has identified some areas of the core competency framework for specialist nurses, including clinical care delivery, leadership and management, ethical decision-making, expert guidance, and the ability to conduct clinical research, provide consultations, and collaborate with others. It is also important to emphasize that direct clinical care provision is a central aspect of specialist nurses’ roles, distinguishing them from individuals involved in nursing education or management. In the context of the American Nurses’ Association assessment of nurses’ competencies, the content of the modified Six-Sigma-based training program is mainly based on scoring learners’ core competencies, theoretical knowledge, operational skills, clinical nursing lectures, reviews, and nursing case management skills [20].
The Six Sigma methodology is an American innovation based on the development of total quality management [21]. This approach includes many pioneering achievements at the forefront of management and is a rigorous, focused, and efficient method to improve a company’s process management quality [22]. Six Sigma management is a process-advancing method rather than a quality program and can be used to analyze processes, quantify process characteristics from the status quo to the target, identify process goals and requirements, and discover methods and entry points for quality improvement [23]. Shah & Emerick [24] advocated the future use of Six Sigma to ensure patient safety, acquire quality improvements in anesthesiology, and address the growing healthcare-related challenges. Pocha [25] applied Six Sigma tools to optimize the nursing management process and improve patient satisfaction. Reportedly, lean Six Sigma techniques can reduce the duration and variability of patient inclinic time and increase service capacity in outpatient ophthalmology clinics without additional resource input [26]. Davidson et al. [27] pointed out that this methodology is also beneficial for continuous quality improvement in the education field and summarized the critical success sectors and barriers of Lean Six Sigma in higher education. Vaughn et al. [28] used the Six Sigma define, measure, analyze, improve, and control (DMAIC) strategy as a systematic approach to root cause analysis in their quality improvement course for orthopedic residents and achieved good results.
Therefore, to promote the popularization and development of rehabilitation specialist nurses, as well as enhance the quality of their training, the rehabilitation specialist nurse training base in Hunan Province adopted the Six Sigma method in a teaching reform to explore the effects of short-term rehabilitation specialist nurse training and provide valuable insights for developing countries and distressed areas.
2. Purpose and hypothesis
The purpose of this study was to examine the effect of the modified Six-Sigma-based training program against a conventional educational program on rehabilitation specialist nurses’ core competencies scores, post-training performance, and satisfaction.
The hypotheses are as follows: The modified training program based on the Six Sigma methodology is likely to improve rehabilitation nurses’ training satisfaction and enhance the cultivation of their core competencies.
METHODS
1. Study design
The DMAIC process improvement method is an important part of the Six Sigma methodology and defines concrete interventions based on five steps: definition, measurement, analysis, improvement, and control. The duration of the intervention in this study was two months, that is, one month each for clinical practice and theoretical lectures, of which clinical practice was seven hours a day, five days a week, while theoretical lectures were forty-five minutes per session, two credit hours per course. Through the five steps of the Six Sigma DMAIC strategy, we improved training quality in three aspects: base management, theoretical teaching, and practical training.
2. The modified six-sigma-based training program
1) Definition phase
Identify critical to quality (CTQ) characteristics that affect product quality, performance, customer satisfaction, process improvement needs, and targets for improvement.
The Six Sigma methodology teaching reform team was composed of the head teacher, director of the practical base, director of the theoretical base, and all the teachers who participated in the course. The head teacher was responsible for collecting data on learners’ satisfaction with the courses and teachers and evaluating the learners’ core competencies. The teachers were responsible for providing feedback on learners’ classroom performance, and the directors of the theoretical and practical bases were responsible for coordinating and organizing the reform of the teaching plan. The detailed training project charter consisting of questions, targets, and CTQ attributes was used. The targets of the teaching reform included meeting the learners’ learning needs, improving learners’ satisfaction, and improving their core competencies as rehabilitation specialist nurses. The CTQ of the education reform focused on the latter two.
2) Measurement phase
Measure the process, establish the baseline and expected goals, and compare effectiveness before and after implementation.
During the measurement phase, we collected both learners’ and teachers’ opinions and suggestions regarding the rehabilitation specialist nurses’ training before and after the educational reform to identify the deficiencies in the training.
The following data were collected for each learner:
• Demographic data, including age, years of work experience, designation, work department, educational background, and professional title.
• Specialist nurses’ core competencies.
• Rehabilitation specialist nurses’ satisfaction with training.
• Theoretical knowledge, operational skills, reviews, clinical nursing lectures and nursing case management scores.
3) Analysis phase
Utilize statistical analysis tools to analyze the data collected to identify the critical factors influencing the process.
In this phase,we have compiled the opinions and suggestions of learners and teachers and conducted a teaching analysis meeting for rehabilitation specialist nurses to identify the reasons for the problems in the training of rehabilitation specialist nurses in recent years. We summarized the problems and reasons from three aspects and proposed countermeasures: training base management, theoretical teaching, and practical training. Further details are listed in Table 1.
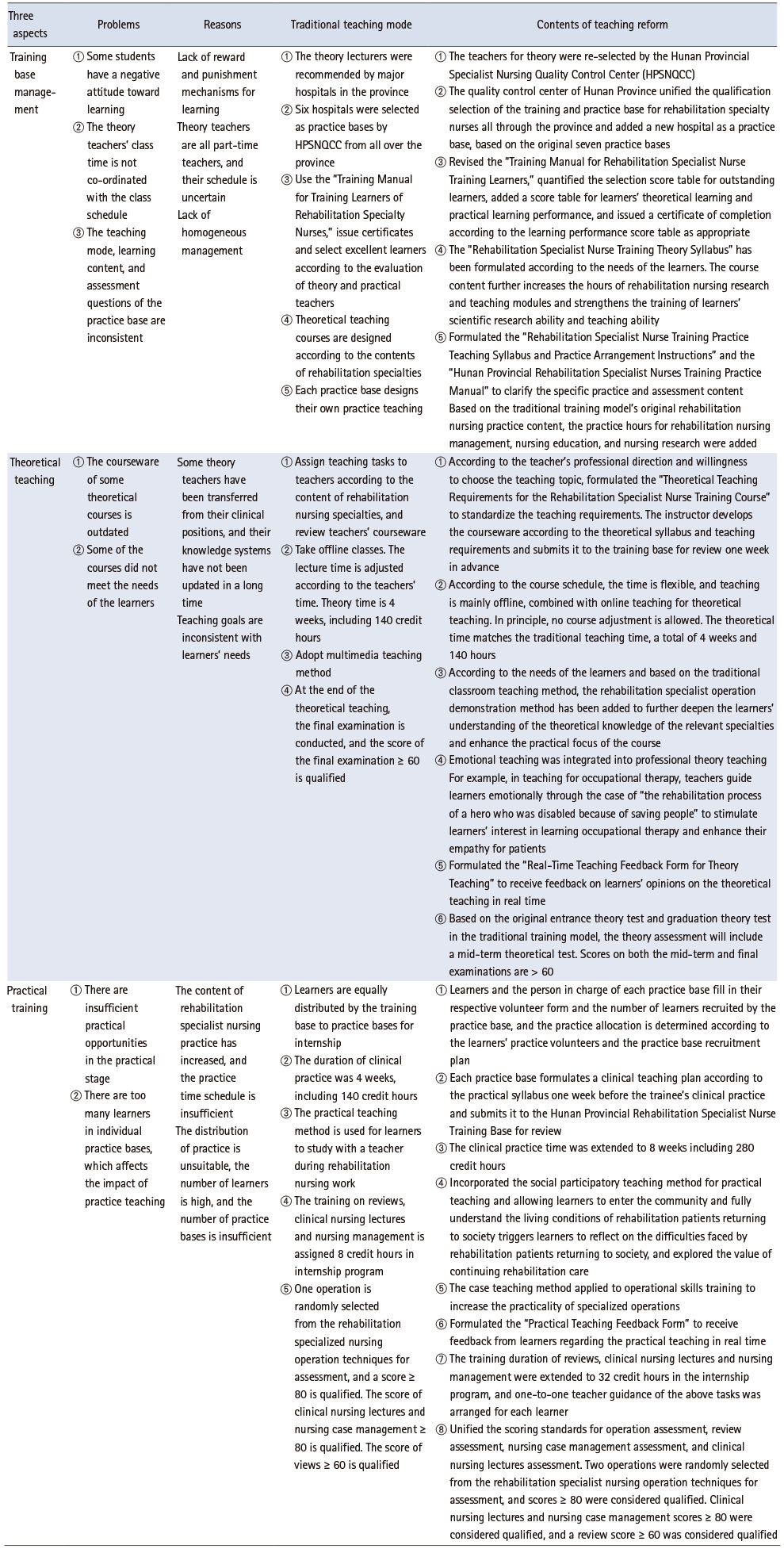
Table 1
Analysis of Deficiencies in the Training of Rehabilitation Specialist Nurses and Training and Teaching Reform Program for Rehabilitation Specialist Nurses
4) Improvement phase
Discover ways to eliminate or reduce critical influence factors, evaluate implementation risks, and verify the effectiveness of improvements.
We proposed solutions to solve the problems in traditional teaching mode that emerged from the analysis. We unified each suggested aspect and formulated the best improvement plan, which included optimizing workflows and designing focused training programs for difficult problems. The details of the training and teaching reform programs for rehabilitation specialist nurses are shown in Table 1.
5) Control phase
Development of a control plan and definition of monitoring methods to sustain improvements and achieve the desired objectives.
The researchers organized seminars for learners to collect real-time feedback on teaching training and adjusted the training plan according to real-time teaching feedback and seminars. Some training plans would be adjusted based on the the feedback to ensure the reform plan is implemented according to the Six Sigma method.
Emphasis was placed on skills assessment, and the evaluation indicators of training effectiveness included theoretical knowledge, operational skills, clinical nursing lectures, reviews, nursing case management, core competencies for rehabilitation specialist nurses, and trainee satisfaction.
3. Setting and sample
This study was conducted as a quasi-randomized controlled trial organized by the government during the 2020 and 2021 academic years, with a limited number of participating trainees. All students attending the training course at Hunan Provincial Rehabilitation Specialist Nurse Training Base (HRSNTB) were eligible for participation, and there were no exclusion criteria for learners. The control group consisted of 56 learners who participated in the 2020 training course at the HRSNTB, whereas the intervention group included 60 learners from the HRSNTB’s 2021 training course. In total, 116 participants were included in the study. All participants were fully engaged in the study and there were no drop-outs during the five steps. The data were collected in the same way for both groups after implementing the modified Six-Sigma-based training program. The effects of these two methods on the rehabilitation specialist nurses’ training were compared by evaluating the nurses’ pre- and post-intervention core competencies and satisfaction scores. The learners’ performance in terms of theoretical knowledge, operational skills, reviews, clinical nursing lectures, and nursing case management post-training was also compared between the two groups. All the learners participated voluntarily in this training and no ethical issues arose. As shown in Table 2, all 116 learners originally in the study completed training and acquired rehabilitation specialist nursing certifications. There were no statistically significant differences in the basic data between the two groups (p > .05).
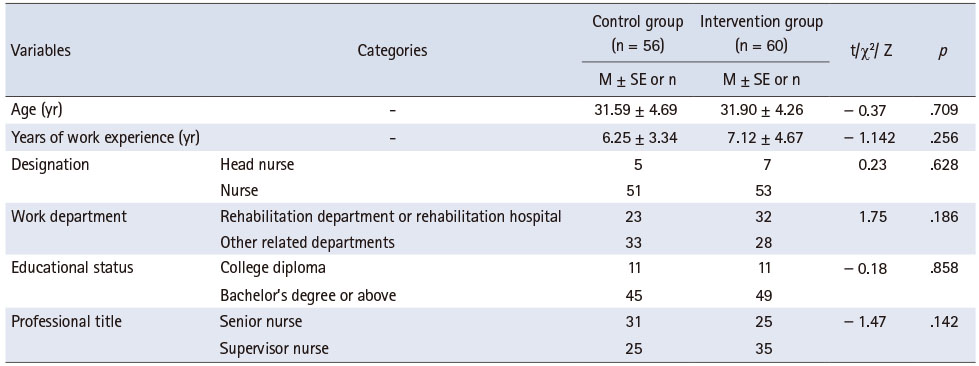
Table 2
Comparison of Basic Information of the Two Groups of Participants
4. Data collection
1) General information questionnaire
The general information questionnaire included questions on age, years of work experience, designation, work department, educational background, and professional title.
2) Core competency questionnaire
The questionnaire was compiled by Wang [29] and includes 69 items: 8 first-level indexes, 21 second-level indexes, and 66 third-level indexes. The first-level indexes include professional rehabilitation nursing ability, educational guidance ability, ability to communicate and collaborate, critical thinking skills, professional development capability, professional quality, ability to support and supervise, and rehabilitation nursing management ability. Professional rehabilitation nursing ability includes the ability to acquire knowledge about rehabilitation and other relevant professional knowledge, and the ability to perform rehabilitation techniques; it contains 23 questions. Educational guidance ability includes health education, clinical teaching, and rehabilitation guidance competencies; it contains 11 questions. The ability to communicate and collaborate includes communication and teamwork skills and contains seven questions. Critical thinking skills include rehabilitation assessment skills, analytical decision-making skills, and rehabilitation evaluation skills, and contains eight questions. Professional development capability includes the ability to innovate in nursing research and personal professional development and contains five questions. Professional quality includes professional identity, empathy, and responsibility, and contains three questions. The ability to support and supervise includes encouraging support and monitoring guidance and contains five questions. Rehabilitation nursing management ability includes planning, organizational and coordination, and quality control skills in rehabilitation care; it contains seven questions. The items were answered using a 5-point Likert scale (5 = completely agree, 4 = basically agree, 3 = uncertain, 2 = basically disagree, and 1 = totally disagree). The Cronbach’s α coefficient of the questionnaire’s overall index system was .966. The Cronbach’s α coefficient of the first-level index was between .805 and .948 and that of the second-level index was between .714 and .983.
3) Training satisfaction questionnaire
We used a satisfaction questionnaire designed by the researcher to assess the rehabilitation nurses’ satisfaction with their training. The researchers selected the following four items to explain rehabilitation nurses’ satisfaction: (1) overall satisfaction, (2) satisfaction with base management, (3) satisfaction with theoretical instruction, and (4) satisfaction with clinical practice. Each question was graded on a scale of 1~2 points, 1 meaning “satisfactory” and 2 meaning “fair/unsatisfactory.” The reliability of this study was Cronbach’s α = 0.987.
4) Scores for operational skills, theoretical knowledge, reviews, clinical nursing lectures, and nursing case management
The difficulty levels of the two groups’ theoretical knowledge tests were the same, and we adopted a unified scoring standards system (100-point) to assess operational skills, reviews, clinical nursing lectures, and nursing case management. The learners’ theoretical knowledge, operational skills, clinical nursing lectures, and nursing case management scores had to reach at least 80 points, and the learners’ reviews required a score of at least 60 points. The assessment papers for theoretical knowledge, operational skills, clinical nursing lectures, reviews, and nursing case management were developed in strict accordance with the requirements of the Nursing Teaching Assessment Regulations. The investigators were uniformly trained.
5. Data analysis
Statistical analyses were performed using SPSS Statistics (version 22.0, IBM, Armonk, NY, USA) software. Categorical data are presented as case counts and percentages, and a t-test or rank sum test was used for comparisons between the two groups. Measurement data were represented by (
The core competencies of the rehabilitation specialist nurses in the two groups were evaluated using directly distributed paper questionnaires for surveys from pre- to post-test. Differences in training satisfaction between the two groups of learners after training were also evaluated. After training, operational skills, theoretical knowledge, reviews, clinical nursing lectures, and nursing case management were compared between the two groups.
6. Ethics considerations
All study participants were trainees of the HRSNTB who gave their informed consent to the study content and specific assessment indicators, which were collected in terms of age, years of work experience, work sector, educational background, and title, and assessment indicators, including theoretical knowledge, operational skills, clinical nursing lectures, reviews, and nursing case management scores. The study was conducted in accordance with the Declaration of Helsinki and approved by the Research Ethics Committee (No. LC2022105).
RESULTS
1. Core competencies
After the modified Six-Sigma-based training program, participants in the intervention group showed significant improvement on all the core competencies. Compared to the control group, the intervention group showed significant improvement in professional rehabilitation nursing ability (t = 16.83, p < .001), critical thinking skills (t = 20.99, p < .001), educational guidance ability (t = 16.61, p < .01), ability to support supervision (t = 18.04, p < .001), ability to communicate and collaborate (t = 19.61, p < .001), rehabilitation nursing management ability (t = 14.74, p < .001), professional development capability (t = 2.16, p = .03), and professional quality (t = 13.89, p < .001) following the intervention. Moreover, the participants in the intervention group showed significant improvement in professional rehabilitation nursing ability (t = 25.92, p < .001), critical thinking skills (t = 18.17, p < .001), educational guidance ability (t = 21.41, p < .001), ability to support supervision (t = 24.66, p < .01), ability to communicate and collaborate (t = 21.07, p < .001), rehabilitation nursing management ability (t = 14.67, p < .001), professional development capability (t = 5.32, p < .001), and professional quality (t = 22.12, p < .001) between the pre- and posttests (see Table 3).
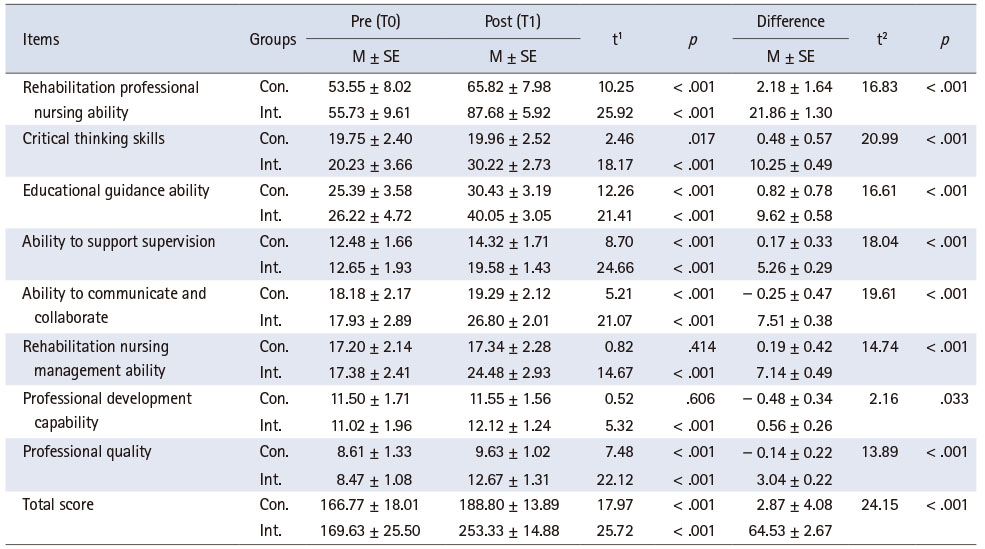
Table 3
Comparison of the Scores of the Core Competencies of Rehabilitation Specialist Nurses between the Two Groups
2. Professional competence
All the participants completed the training program. In Figure 1, the scores (labeled on the y-axis) are broken down by each of the five aspects (labeled on the x-axis). The scores per aspect are represented on the graph, with the boxes indicating interquartile deviation and the marker in the middle of the box indicating the median score. The dotted lines or “whiskers” protruding from the top and bottom of the boxes indicate the minimum and maximum scores for the five aspects of the participants. Additionally, operational skills, reviews, and clinical nursing lectures each have one outlier represented on the graph by small dots at the low end of the scores. At the time of intervention termination, the scores for theoretical knowledge, reviews, clinical nursing lectures, and nursing case management were significantly higher in the intervention group than in the control group (p < .05), while operational skills scores were not statistically significantly different between the two groups (Z = -1.42, p = .156).
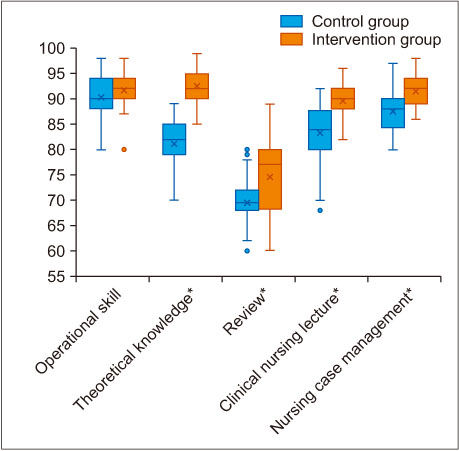
Figure 1
Comparison of scores of operational skill, theoretical knowledge, reviews, clinical nursing lectures, and nursing case management. *p < 0.05.
3. Satisfaction with the training
As shown in Table 4, at the time of the intervention, base management satisfaction, theoretical teaching satisfaction, and overall satisfaction were significantly higher in the intervention group than in the control group (p < .05), while the difference in the clinical practice satisfaction scores between the two groups was not significant.
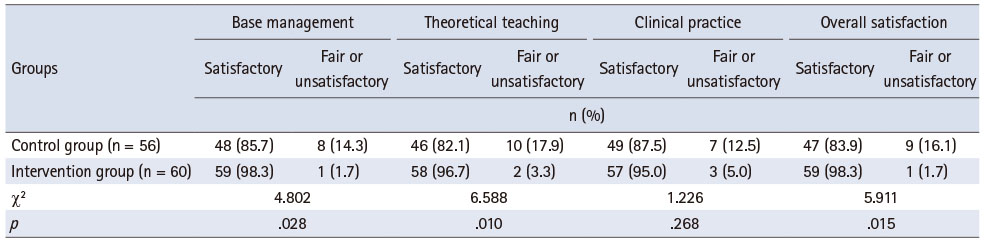
Table 4
Comparison of Degree of Satisfaction between the Two Groups of Learners after Training
DISCUSSION
1. Improvement in the core competencies
Although studies have investigated the effects of training programs on teaching clinical skills in rehabilitation nursing [13], few have discussed the training effectiveness of core competencies for specialized nurses. A systematic and professional rehabilitation nursing education program is important to promote nurses’ understanding of and professional development in the rehabilitation nursing profession. The results of this study show that the conventional teaching model was not effective in improving learners’ rehabilitation nursing management and professional development abilities, while the modified Six-Sigma-based training program promoted all dimensions of the rehabilitation specialist nurses’ core competencies. This is consistent with the study by Xiao et al. [30], which showed that the Six Sigma methodology can improve teaching quality in pediatric nurse training. A study conducted at a private hospital in Ireland demonstrated that the introduction of the Six Sigma model into a basic life support training program for medical staff led to improved satisfaction among participants. Furthermore, the study revealed that the implementation of the Six Sigma model significantly reduced the training time and costs for both the training departments and instructors involved [31].
The defects and deficiencies existing in conventional teaching were fully understood in the measurement- and-analysis stage of the Six Sigma management model, and teaching evaluation was standardized during the improvement stage [26], which resulted in improved teaching quality. Moreover, various assessment indicators were unified and quantified to ensure the scientific nature and rationality of the teaching effect evaluation. Standardized teaching evaluation has been widely implemented in nurse training programs across many countries because it provides an effective and objective method for assessing teaching effectiveness [32, 33]. Furthermore, in the improvement stage, the practice content of the relevant core competencies was added to the practice outline to ensure that training for various core competencies, such as education guidance, rehabilitation nursing management, and professional development abilities, was no longer limited to theory. In addition, a teaching feedback mechanism was established throughout the training to allow theoretical and practical teachers to reflect on and adjust their teaching plans in a timely manner, which promoted improvements in teaching quality.
We extended the training period for education reform. After completing the modified Six-Sigma-based training program, the rehabilitation specialist nurses’ core competencies achieved a marked improvement.
2. Improvement in professional competence
Specialist nurses are practitioners and promoters of professional development [34] who teach and conduct scientific research in clinical nursing work; therefore, improving their professional development abilities is of great importance. In this teaching reform, the scores for theoretical knowledge, reviews, clinical nursing lectures, and nursing case management for the intervention group were significantly higher than that for the control group. This is mainly due to the following reasons. First, we focused on stimulating the nurses’ active learning potential, adhering to problem-oriented teaching methods, and stimulating their desire for learning and exploration, which created a dynamic and innovative learning atmosphere. Thus, learners’ initiative and enthusiasm for learning increased significantly.
Second, in view of the learners’ weak abilities in reviews, clinical nursing lectures, and nursing case management, we provided scientific research nursing lectures throughout the training process to renew their knowledge structure and cultivate critical thinking ability. We extended the credit hours in this part of the training to ensure the teaching effect. We also implemented a one-to-one tutorial system to provide effective guidance for learners, which helped resolve their issues in a timely manner and improve their performance, consistent with the research of Qi & Wang [35]. Their study showed that the application of a “one-to-one” tutorial system combined with reflective teaching in nursing education for the intensive care department can significantly improve the nurses’ theoretical knowledge and operational skills in routine training and is conducive to improving their critical thinking ability.
Third, we paid special attention to students’ oral expression, teaching, and clinical thinking abilities. During the teaching process, we purposefully and relevantly arranged special discussions, special lectures, and health education lectures. We applied the case teaching method to operational training to increase the practicality of specialized operations and required learners to manage typical clinical cases throughout the course. In recent years, several countries have integrated clinical cases into training programs for specialized nurses [36, 37, 38], with the aim of enhancing their problem-solving abilities and bridging the gap between the teaching environment and real-world clinical settings [39]. In the process of clinical case management, we required learners to participate in nursing evaluations, diagnoses, treatment plans, and measures of clinical cases, as well as to track the nursing outcomes of patients. Finally, we summarized and reported the experience of managing the entire case. In this way, the learners’ clinical thinking and practical abilities significantly improved.
Compared with the conventional educational program, the modified Six-Sigma-based training program did not result in a higher operational skills score. Objective structured assessment reflects specialist nurses’ true operational levels and resilience in clinical applications [40]. In this study, we used traditional assessment methods after the teaching reforms. In future research, we need to discuss the impact of assessment methods on outcomes.
In addition, the duration of professional practice teaching was extended from one to two months, with the purpose of improving the clinical application of professional competence in rehabilitation, and the score of the intervention group in terms of nursing case management was significantly improved after the training program. This is consistent with the findings of a previous study [41]. As learning time is an important factor influencing learning outcomes [42, 43], these results suggest that future research should consider the best learning time when developing training programs to increase the effect of training.
3. Improvement in the learners’ satisfaction with the training
Learners’ satisfaction with the training is an indicator of the teaching effect. This study determined that the use of the modified Six-Sigma-based training program for rehabilitation specialist nurses was more beneficial than the use of conventional educational programs regarding training satisfaction, including base management and theoretical teaching.
This is possible for several reasons. First, the Six-Sigma-based education method strengthened the learners’ reward and punishment mechanisms, which increased their learning enthusiasm. Second, the application of emotional teaching in theoretical teaching allowed learners to understand the value of rehabilitation nursing and enhance their professional identity [44]. Third, the operational demonstration teaching method was added to the theoretical courses, fully combining theory and practice and increasing the interest and practicability of training courses [45]. Finally, we respected the feedback of the learners throughout the training and adjusted our teaching methods and content accordingly.
However, the improvement in clinical practice satisfaction was not significant, mainly because of the following reasons: First, the learners in the two groups were from different departments; only 41.1% to 53.3% of the learners were from rehabilitation departments in our education program; therefore, the learning focus and needs of learners were diversified. Furthermore, in the clinical practice stage, we chose different hospitals as clinical practice bases, resulting in uneven teaching levels and affecting the learners’ satisfaction with the clinical practice. Moreover, different teaching bases adopt different teaching methods; some clinical teaching bases still use conventional teaching modes, which cannot meet the diverse learning needs of learners. Although the clinical practice teaching syllabus and manual have been unified, some clinical practice teaching bases have also introduced social participatory teaching, which has been shown to stimulate learners’ empathy and improve their learning interest and communication abilities [46]. However, this type of teaching does not apply to all practice bases. Researchers have also found that diversified teaching methods such as clinical practice teaching, simulated ward teaching, and case teaching are more convenient for deepening learners’ understanding and improving their memory [47, 48]. In future, these practical teaching modes should be implemented to solve this problem.
4. Limitations
There were some limitations in the process of this specialty nursing teaching reform. First, we primarily focused on the improvement of theoretical knowledge and core competencies. Thus, the effect of training on rehabilitation practice was not apparent and needs to be further strengthened. Second, the learners’ clinical practice ability was assessed via specialist operation skills, but a gap remains between theory and practice. In the next step, we will continue to explore ways to improve specialist nurses’ clinical practice training. Third, the control and intervention training sessions were held at different times, approximately a year apart, which may have affected the accuracy of the results. Future research should include more participants and apply teaching reforms to different regions to verify their effectiveness.
CONCLUSION
The training and teaching reform plan for rehabilitation specialist nurses based on the Six Sigma management model strengthened training base management; expanded the breadth, depth, and practicability of and interest in theoretical courses; implemented homogeneous management of clinical practice; updated teaching methods; and enhanced the training effect on learners’ core competencies. However, the management and training of practice bases need to be strengthened, a more effective and suitable practice training model for rehabilitation specialist nursing should be further explored, and the clinical practice teaching effect and students’ satisfaction with practice learning should continue to be improved.
Notes
CONFLICTS OF INTEREST:The authors declared no conflict of interest.
AUTHOR CONTRIBUTIONS:
Conceptualization or/and Methodology: Gu JY & Luo L.
Data curationn or/and Analysis: Ma SM & Li CJ.
Funding acquisition: None.
Investigation: Gu JY & Luo L & Li CJ & Ma SM & Gong FH.
Project administration or/and Supervision: Gong FH.
Resources or/and Software: Gu JY & Ma SM & LI CJ.
Validation: Gu JY.
Visualization: Gu JY.
Writing original draft or/and Review & Editing: Gu JY & Luo L & LI CJ & Ma SM & Gong FH.
ACKNOWLEDGEMENTS
None.
DATA SHARING STATEMENT
Please contact the corresponding author for data availability.
References
-
National Health and Family Planning Commission of the People’s Republic of China. [National Nursing Development Plan (2016–2020)]. Chinese Nursing Management 2017;17(1):1–5. [doi: 10.3969/j.issn.1672-1756.2017.01001]Chinese.
-
-
Jin Y, Xu XD. The development status of stroke rehabilitation nursing. Chinese Nursing Management 2018;18(6):726–729.
-
-
Shi RY, Qu BL, Li HY, Kang LH, Kong XC. Rehabilitation resource and rehabilitation nursing needs of patients at home in Xuzhou. Chinese Journal of Modern Nursing 2020;26(8):1019–1024. [doi: 10.3760/cma.j.cn115682-20190912-03317]
-
-
Wang Y, Weng YL, Zhou LS. Role orientation of specialty nurses in rehabilitation. Chinese Journal of Nursing Education 2019;16(9):657–661. [doi: 10.3761/j.issn.1672-9234.2019.09.004]
-
-
Meng X, Chen X, Liu Z, Zhou L. Nursing practice in stroke rehabilitation: Perspectives from multi-disciplinary healthcare professionals. Nursing & Health Sciences 2020;22(1):28–37. [doi: 10.1111/nhs.12641]
-
-
Zhan LL, Yao L, An L, Feng JJ, Shang WH, Li W, et al. Enlightenment of typical national rehabilitation nursing service mode. Chinese Health Quality Management 2022;29(4):1–3. 8, 120. [doi: 10.13912/j.cnki.chqm.2022.29.04.01]
-
-
Meng L, Li XY, Zheng CE. The training program construction and practice of clinical nurse specialists in rehabilitation nursing. Chinese Nursing Management 2018;18(6):730–732. [doi: 10.3969/j.issn.1672-1756.2018.06.003]
-
-
Chen JJ, Mei SL, Jiang HY, Du C. Application of PDCA cycle in management of teaching quality of rehabilitation nurse. Chinese Journal of Rehabilitation Theory and Practice 2016;22(10):1232–1235. [doi: 10.3969/j.issn.1006-9771.2016.10.026]
-
-
Wu GL, Yang MY, Bao JH, Ni H, Song G, Xu W, et al. Practice and exploration of standardized training for nurses in rehabilitation nursing of Yunnan Province. Journal of Kunming Medical University 2019;40(6):140–143. [doi: 10.3969/j.issn.1003-4706.2019.06.029]
-
-
Wang X, Meng L, Li XY. Training program for clinical nurse specialists in rehabilitation nursing. Journal of Nursing Science 2018;33(20):65–66.
-
-
Ding YM, Wu XJ, Wang XY, Xiao Y, Deng J, Tian J, et al. Investigation on training of specialized nurses developed by nursing associations at all levels in China. Chinese Journal of Nursing 2020;55(5):747–750. [doi: 10.3761/j.issn.0254-1769.2020.05.023]
-
-
Li CJ, Teng LY. [Investigation and analysis on the demand for standardized training of rehabilitation nurses]. Beijing Medical Journal 2021;43(1):92–94. [doi: 10.15932/j.0253-9713.2021.01.027]Chinese.
-
-
Jokiniemi K, Miettinen M. Specialist nurses’ role domains and competencies in specialised medical healthcare: A qualitative descriptive study. International Journal of Caring Sciences 2020;13(1):171–179.
-
-
Zhao JW, Fang YG, Li YJ. [Effective management of clinical nursing specialists and specialist nurses]. Nanfang Journal of Nursing 2005;(3):21–23. [doi: 10.16460/j.issn1008-9969.2005.03.010]Chinese.
-
-
Guspianto, Asyary A, Ibnu IN. Integration model of total quality management and six sigma in hospital quality management. Management Science Letters 2021;11(4):1439–1442. [doi: 10.5267/j.msl.2020.10.014]
-
-
Tlapa D, Tortorella G, Fogliatto F, Kumar M, Mac Cawley A, Vassolo R, et al. Effects of lean interventions supported by digital technologies on healthcare services: A systematic review. International Journal of Environmental Research and Public Health 2022;19(15):9018 [doi: 10.3390/ijerph19159018]
-
-
Davidson JM, Price OM, Pepper M. Lean Six Sigma and quality frameworks in higher education – a review of literature. International Journal of Lean Six Sigma 2020;11(6):991–1004. [doi: 10.1108/IJLSS-03-2019-0028]
-
-
Vaughn NH, Hassenbein SE, Black KP, Armstrong AD. Important elements in the quality improvement curriculum for orthopaedic residents. Journal of Bone and Joint Surgery. American Volume 2019;101(7):e28 [doi: 10.2106/JBJS.18.00061]
-
-
Wang HM. In: Construction of core competence evaluation index system for rehabilitation nurse specialists [master’s thesis]. Qingdao: Qingdao University; 2019. pp. 1-102.
-
-
Xiao N, Shi SN, Xie JH, Zhu LH, Liu Y. The effect of DMAIC based training on quality improve in pediatric specialized nurses. Chinese Nursing Management 2018;18(2):218–223. [doi: 10.3969/j.issn.1672-1756.2018.02.016]
-
-
Dempsey A, Robinson C, Moffatt N, Hennessy T, Bradshaw A, Teeling SP, et al. Lean Six Sigma redesign of a process for healthcare mandatory education in basic life support-a pilot study. International Journal of Environmental Research and Public Health 2021;18(21):11653 [doi: 10.3390/ijerph182111653]
-
-
Olsen JM, Lagunas MCW, Wildenberg C, Sohn KM, Brenner GH, Jadack RA, et al. Using standardized exams for formative program evaluation. Teaching and Learning in Nursing 2021;16(4):371–374. [doi: 10.1016/j.teln.2021.06.006]
-
-
Qi ZL, Wang F. The application of “one-to-one” tutor system in ICU nurse teaching. China Continuing Medical Education 2020;12(2):28–30. [doi: 10.3969/j.issn.1674-9308.2020.02.012]
-
-
Zheng SD, Li JZ. SWOT analysis of case-based teaching in nursing education. Education Modernization 2019;6(68):181–184. 190. [doi: 10.16541/j.cnki.2095-8420.2019.68.062]
-
-
Aluisio AR, Daniel P, Grock A, Freedman J, Singh A, Papanagnou D, et al. Case-based learning outperformed simulation exercises in disaster preparedness education among nursing trainees in India: A randomized controlled trial. Prehospital and Disaster Medicine 2016;31(5):516–523. [doi: 10.1017/S1049023X16000789]
-
-
van den Beemt A, van de Watering G, Bots M. Conceptualising variety in challenge-based learning in higher education: The CBL-compass. European Journal of Engineering Education 2023;48(1):24–41. [doi: 10.1080/03043797.2022.2078181]
-
-
Di HD, Chen L, Wang F, Lyu L, Liu N, Sheng LXB. Application of objective structured clinical examination assessment mode in neurosurgery specialist nurse training. Chinese Journal of Practical Nursing 2022;38(28):2196–2202. [doi: 10.3760/cma.j.cn211501-20210305-00655]
-
-
Kaswan MS, Rathi R. Analysis and modeling the enablers of Green Lean Six Sigma implementation using Interpretive Structural Modeling. Journal of Cleaner Production 2019;231:1182–1191. [doi: 10.1016/j.jclepro.2019.05.253]
-
-
Meyer E, Van Klaveren C. The effectiveness of extended day programs: Evidence from a randomized field experiment in the Netherlands. Economics of Education Review 2013;36:1–11. [doi: 10.1016/j.econedurev.2013.04.002]
-
-
Kikuchi N. The effect of instructional time reduction on educational attainment: Evidence from the Japanese curriculum standards revision. Journal of the Japanese and International Economies 2014;32:17–41. [doi: 10.1016/j.jjie.2014.01.001]
-
-
Su SD. Application of operation point demonstration method in nursing practical teaching. Contemporary Nurses (The next ten-day Issue) 2018;25(10):164–166.
-
-
Pulimeno M, Piscitelli P, Miani A, Colazzo S, Mazza A, Colao A. Narrative pedagogy to promote health and wellbeing in school setting: An approach proposed by UNESCO chair on health education and sustainable development. Health Promotion Perspectives 2020;10(1):1–2. [doi: 10.15171/hpp.2020.01]
-
-
Björklund K, Silén C. Occupational therapy and physiotherapy students’ communicative and collaborative learning in an interprofessional virtual setting. Scandinavian Journal of Occupational Therapy 2021;28(4):264–273. [doi: 10.1080/11038128.2020.1761448]
-
 Cite
Cite
