 Submit an article
Submit an article
Articles
- Page Path
- HOME > J Korean Acad Nurs > Volume 55(4); 2025 > Article
-
Review Paper
노인의 디지털헬스리터러시 관련 변인: 체계적 문헌 고찰 및 메타분석 -
박진화
 , 문은주
, 문은주 - Variables influencing digital health literacy in older adults: a systematic review and meta-analysis
-
Jin Hwa Park, Eun Ju Mun
-
Journal of Korean Academy of Nursing 2025;55(4):651-667.
DOI: https://doi.org/10.4040/jkan.25112
Published online: November 27, 2025
대구가톨릭대학교 간호대학
College of Nursing, Daegu Catholic University, Daegu, Korea
- Corresponding author: Eun Ju Mun College of Nursing, Daegu Catholic University, 33 Duryugongwon-ro 17-gil, Nam-gu, Daegu 42472, Korea E-mail: quffndi@hanmail.net
• Received: August 6, 2025 • Revised: November 5, 2025 • Accepted: November 5, 2025
© 2025 Korean Society of Nursing Science
This is an Open Access article distributed under the terms of the Creative Commons Attribution NoDerivs License (http://creativecommons.org/licenses/by-nd/4.0) If the original work is properly cited and retained without any modification or reproduction, it can be used and re-distributed in any format and medium.
- 3,393 Views
- 306 Download
- 1 Crossref
Abstract
-
Purpose
- This study aimed to synthesize existing evidence on digital health literacy (DHL) among older adults and to estimate the associations between related influencing factors through a systematic literature review and meta-analysis.
-
Methods
- A systematic review and meta-analysis were conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) and Meta-Analysis of Observational Studies in Epidemiology (MOOSE) guidelines. Literature searches were performed across PubMed, EMBASE, Cochrane Library, CINAHL, RISS, and DBPIA. The search and screening process was conducted from December 24, 2023, to March 31, 2025. Effect sizes (ESr) using correlation coefficient for each variable were calculated, and meta-analyses were performed using Microsoft Excel and R version 4.3.1.
-
Results
- Forty-seven variables were identified, including two demographic, six physical, six behavioral, 23 psychosocial, and 10 cognitive factors. Meta-analysis results showed that physical, behavioral, psychosocial, and cognitive factors had significant effects on DHL. Among these, digital information level (ESr=.62; 95% confidence interval [CI], 0.55 to 0.69) within the cognitive domain and technophobia (ESr=−.55; 95% CI, −0.47 to −0.40) within the psychosocial domain demonstrated the largest ESr.
-
Conclusion
- Among factors influencing DHL, digital information level and technophobia showed the strongest associations. These findings suggest that improving DHL in older adults requires a dual approach targeting both cognitive and psychosocial dimensions—enhancing digital information skills while reducing technophobia—to effectively support digital engagement and health empowerment in this population (PROSPERO registration number: CRD42023487486).
서론
방법
결과
1) 분석 대상 문헌의 일반적 특성
2) 노인의 디지털헬스리터러시 관련 변인
3) 논문의 질 평가
1) 요인별 효과크기
2) DHL 관련 변인들의 효과크기
3) 출판편의에 대한 검정
고찰
결론
-
Conflicts of Interest
No potential conflict of interest relevant to this article was reported.
-
Acknowledgements
None.
-
Data Sharing Statement
Please contact the corresponding author for data availability.
-
Supplementary Data
Supplementary data to this article can be found online at https://doi.org/10.4040/jkan.25112.
Supplementary Figure 1.
jkan-25112-Supplementary-Figure-1.pdf
Supplementary Figure 2.
-
Author Contributions
Conceptualization or/and Methodology: JHP, EJM. Data curation or/and Analysis: JHP, EJM. Funding acquisition: none. Investigation: JHP, EJM. Project administration or/and Supervision: JHP. Resources or/and Software: EJM. Validation: JHP, EJM. Visualization: EJM. Writing: original draft or/and Review & Editing: JHP, EJM. Final approval of the manuscript: all authors.
Article Information
Figure 1.PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow diagram: study selection process. DHL, digital health literacy.

Table 1.Characteristics of studies included in systematic review and meta-analysis
Values are presented as number or mean±standard deviation unless otherwise stated.
CD, chronic disease; CDSM, chronic disease self-management model; CMI, comprehensive model of information looking; COPD, chronic obstructive pulmonary disease; DHL, digital health literacy; DM, diabetes mellitus; EHL, electronic health literacy; IMeHU, integrative model of eHealth use, KAB model, knowledge, attitude, behavior model; NR, not report; TRAM, technology readiness and acceptance model.
Table 2.Classification of factors related to digital health literacy and results of studies
Table 3.Quality assessment of studies
Q1: Were the criteria for inclusion in the sample clearly defined?; Q2: Were the study subjects and the setting described in detail?; Q3: Was the exposure measured in a valid and reliable way?; Q4: Were objective, standard criteria used for measurement of the condition?; Q5: Were confounding factors identified?; Q6: Were strategies to deal with confounding factors stated?; Q7: Were the outcomes measured in a valid and reliable way?; Q8: Was appropriate statistical analysis used?
MR, match rate; Y, yes; N, no.
Table 4.Effect size of related factors for digital health literacy of older people
- 1. Zhu X, Yang F. The association among eHealth literacy, depressive symptoms and health-related quality of life among older people: a cross-section study. Int J Older People Nurs. 2023;18(1):e12497. https://doi.org/10.1111/opn.12497ArticlePubMed
- 2. Zhou W, Cho Y, Shang S, Jiang Y. Use of digital health technology among older adults with cancer in the United States: findings from a National Longitudinal Cohort Study (2015-2021). J Med Internet Res. 2023;25:e46721. https://doi.org/10.2196/46721ArticlePubMedPMC
- 3. Yang K, Hu Y, Qi H. Digital health literacy: bibliometric analysis. J Med Internet Res. 2022;24(7):e35816. https://doi.org/10.2196/35816ArticlePubMedPMC
- 4. Jiang X, Wang L, Leng Y, Xie R, Li C, Nie Z, et al. The level of electronic health literacy among older adults: a systematic review and meta-analysis. Arch Public Health. 2024;82(1):204. https://doi.org/10.1186/s13690-024-01428-9ArticlePubMedPMC
- 5. Estrela M, Semedo G, Roque F, Ferreira PL, Herdeiro MT. Sociodemographic determinants of digital health literacy: a systematic review and meta-analysis. Int J Med Inform. 2023;177:105124. https://doi.org/10.1016/j.ijmedinf.2023.105124ArticlePubMed
- 6. Xie L, Zhang S, Xin M, Zhu M, Lu W, Mo PK. Electronic health literacy and health-related outcomes among older adults: a systematic review. Prev Med. 2022;157:106997. https://doi.org/10.1016/j.ypmed.2022.106997ArticlePubMed
- 7. Kim HS, Sung JH. The influence of digital informatization level, self-efficacy, and social support on digital health literacy in the elderly with cancer. Asian Oncol Nurs. 2022;22(4):255-263. https://doi.org/10.5388/aon.2022.22.4.255Article
- 8. Choukou MA, Sanchez-Ramirez DC, Pol M, Uddin M, Monnin C, Syed-Abdul S. COVID-19 infodemic and digital health literacy in vulnerable populations: a scoping review. Digit Health. 2022;8:20552076221076927. https://doi.org/10.1177/20552076221076927ArticlePubMedPMC
- 9. Leung AY, Parial LL, Tolabing MC, Sim T, Mo P, Okan O, et al. Sense of coherence mediates the relationship between digital health literacy and anxiety about the future in aging population during the COVID-19 pandemic: a path analysis. Aging Ment Health. 2022;26(3):544-553. https://doi.org/10.1080/13607863.2020.1870206ArticlePubMed
- 10. Kim S, Chow BC, Park S, Liu H. The usage of digital health technology among older adults in Hong Kong and the role of technology readiness and eHealth literacy: path analysis. J Med Internet Res. 2023;25:e41915. https://doi.org/10.2196/41915ArticlePubMedPMC
- 11. Wang X, Luan W. Research progress on digital health literacy of older adults: a scoping review. Front Public Health. 2022;10:906089. https://doi.org/10.3389/fpubh.2022.906089ArticlePubMedPMC
- 12. Dunn P, Hazzard E. Technology approaches to digital health literacy. Int J Cardiol. 2019;293:294-296. https://doi.org/10.1016/j.ijcard.2019.06.039ArticlePubMed
- 13. Norman CD, Skinner HA. EHEALS: the eHealth Literacy Scale. J Med Internet Res. 2006;8(4):e27. https://doi.org/10.2196/jmir.8.4.e27ArticlePubMedPMC
- 14. van der Vaart R, Drossaert C. Development of the digital health literacy instrument: measuring a broad spectrum of Health 1.0 and Health 2.0 skills. J Med Internet Res. 2017;19(1):e27. https://doi.org/10.2196/jmir.6709ArticlePubMedPMC
- 15. Son H, Han Y. The effect of digital health literacy, self-efficacy on self-care behaviors among community-dwelling elderly: focusing on Gyeongsangbuk-do. Res Community Public Health Nurs. 2025;36(1):59-72. https://doi.org/10.12799/rcphn.2024.00801Article
- 16. Chang SJ, Jang SJ, Lee H, Kim H. Building on evidence to improve eHealth literacy in older adults: a systematic review. Comput Inform Nurs. 2021;39(5):241-247. https://doi.org/10.1097/CIN.0000000000000674ArticlePubMed
- 17. Shi Y, Ma D, Zhang J, Chen B. In the digital age: a systematic literature review of the e-health literacy and influencing factors among Chinese older adults. Z Gesundh Wiss. 2023;31(5):679-687. https://doi.org/10.1007/s10389-021-01604-zArticlePubMedPMC
- 18. Kim K, Shin S, Kim S, Lee E. The relation between eHealth literacy and health-related behaviors: systematic review and meta-analysis. J Med Internet Res. 2023;25:e40778. https://doi.org/10.2196/40778ArticlePubMedPMC
- 19. Seo HJ. The scoping review approach to synthesize nursing research evidence. Korean J Adult Nurs. 2020;32(5):433-439. https://doi.org/10.7475/kjan.2020.32.5.433Article
- 20. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. https://doi.org/10.1136/bmj.n71ArticlePubMedPMC
- 21. Meta-analysis of observational studies in epidemiology: a proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA. 2000;283(15):2008-2012. https://doi.org/10.1001/jama.283.15.2008ArticlePubMed
- 22. Joanna Briggs Institute. Checklist for systematic reviews and research syntheses: the Joanna Briggs Institute critical appraisal tools for use in JBI systematic reviews [Internet]. Joanna Briggs Institute; c2017 [cited 2024 Mar 25]. Available from: https://jbi.global/sites/default/files/2019-05/JBI_Critical_Appraisal-Checklist_for_Systematic_Reviews2017_0.pdf
- 23. Cohen J. Statistical power analysis for the behavioral sciences. 2nd ed. Routledge; 1988. 400 p.
- 24. Hwang SD. Meta-analysis using R. 2nd ed. Hakjisa; 2020. 384 p.
- 25. Maitra S. Fixed-effect versus random-effect model in meta-analysis: how to decide? Indian J Anaesth. 2025;69(1):143-146. https://doi.org/10.4103/ija.ija_1203_24ArticlePubMedPMC
- 26. Borenstein M. In a meta-analysis, the I-squared statistic does not tell us how much the effect size varies. J Clin Epidemiol. 2022;152:281-284. https://doi.org/10.1016/j.jclinepi.2022.10.003ArticlePubMed
- 27. Kasa AS, Drury P, Traynor V, Lee SC, Chang HR. The effectiveness of nurse-led interventions to manage frailty in community-dwelling older people: a systematic review. Syst Rev. 2023;12(1):182. https://doi.org/10.1186/s13643-023-02335-wArticlePubMedPMC
- 28. Jeong AI, Shin S, Hong E. Factors related to workload of intensive care unit nurses: systematic review and meta-analysis. J Korean Clin Nurs Res. 2023;29(3):296-311. https://doi.org/10.22650/JKCNR.2023.29.3.296Article
- 29. Lee J, Lee EH, Chae D. eHealth literacy instruments: systematic review of measurement properties. J Med Internet Res. 2021;23(11):e30644. https://doi.org/10.2196/30644ArticlePubMedPMC
- 30. Aponte J, Nokes KM. Validating an electronic health literacy scale in an older Hispanic population. J Clin Nurs. 2017;26(17-18):2703-2711. https://doi.org/10.1111/jocn.13763ArticlePubMed
- 31. Stellefson M, Paige SR, Tennant B, Alber JM, Chaney BH, Chaney D, et al. Reliability and validity of the telephone-based eHealth Literacy Scale among older adults: cross-sectional survey. J Med Internet Res. 2017;19(10):e362. https://doi.org/10.2196/jmir.8481ArticlePubMedPMC
- 32. Lin CY, Broström A, Griffiths MD, Pakpour AH. Psychometric evaluation of the Persian eHealth Literacy Scale (eHEALS) among elder Iranians with heart failure. Eval Health Prof. 2020;43(4):222-229. https://doi.org/10.1177/0163278719827997ArticlePubMed
- 33. Xie L, Mo PK. Comparison of eHealth Literacy Scale (eHEALS) and Digital Health Literacy Instrument (DHLI) in assessing electronic health literacy in Chinese older adults: a mixed-methods approach. Int J Environ Res Public Health. 2023;20(4):3293. https://doi.org/10.3390/ijerph20043293ArticlePubMedPMC
- 34. Kim H, Yang E, Ryu H, Kim HJ, Jang SJ, Chang SJ. Psychometric comparisons of measures of eHealth literacy using a sample of Korean older adults. Int J Older People Nurs. 2021;16(3):e12369. https://doi.org/10.1111/opn.12369ArticlePubMed
- 35. Oh SS, Kim KA, Kim M, Oh J, Chu SH, Choi J. Measurement of digital literacy among older adults: systematic review. J Med Internet Res. 2021;23(2):e26145. https://doi.org/10.2196/26145ArticlePubMedPMC
- 36. Kim KS. A study of non-probability sampling methodology in sample surveys. Surv Res. 2017;18(1):1-29. https://doi.org/10.20997/SR.18.1.1Article
- 37. Li Q, Fang F, Zhang Y, Tu J, Zhu P, Xi L. eHealth literacy and its outcomes among postsecondary students: systematic review. J Med Internet Res. 2025;27:e64489. https://doi.org/10.2196/64489ArticlePubMedPMC
- 38. Ryu S, Chae Y. The impact of e-health literacy and technological self-efficacy on older adults’ level of digital informatization. J Health Info Stat. 2024;49(4):348-356. https://doi.org/10.21032/jhis.2024.49.4.348Article
- 39. Luo D, Li J, Wang C, Shi Y, Guo HQ, Guang Duan Z. Influence of social support on technophobia in older adults in urban communities: the mediating role of self-efficacy and e-health literacy, a cross-sectional study. BMJ Open. 2025;15(2):e093107. https://doi.org/10.1136/bmjopen-2024-093107ArticlePubMedPMC
- 40. Wang Y, Song Y, Zhu Y, Ji H, Wang A. Association of eHealth literacy with health promotion behaviors of community-dwelling older people: the chain mediating role of self-efficacy and self-care ability. Int J Environ Res Public Health. 2022;19(10):6092. https://doi.org/10.3390/ijerph19106092ArticlePubMedPMC
- 41. Cai S, Du J, Chen X, Li E, Chen Y. The relationship between e-health literacy and educational participation motivation among elderly individuals: the chained mediating effects of self-identity and social capital. Br J Hosp Med (Lond). 2024;85(9):1-13. https://doi.org/10.12968/hmed.2024.0261ArticlePubMed
- 42. Lee JE. Comparative analysis of successful aging in young-old and old-old adults based on Rowe and Kahn’s model: a secondary data analysis. J Korean Gerontol Nurs. 2024;26(2):203-211. https://doi.org/10.17079/jkgn.2024.00325Article
- 43. Cao C, Cao W, Zheng X, Ji K, Wu Y, Hu Z, et al. Association of social capital with self-perceived eHealth literacy among community-dwelling older people: age and gender differences. Front Public Health. 2023;11:1088863. https://doi.org/10.3389/fpubh.2023.1088863ArticlePubMedPMC
- 44. Simmonds M. Quantifying the risk of error when interpreting funnel plots. Syst Rev. 2015;4:24. https://doi.org/10.1186/s13643-015-0004-8ArticlePubMedPMC
References
Appendix
Appendix 1.
Appendix 2.
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
- 고령자를 위한 디지털 헬스 리터러시 측정척도의 적합도 검증
소윤 이
The Korean Journal of Physical Education.2026; 65(2): 157. CrossRef
 ePub Link
ePub Link Cite
CiteVariables influencing digital health literacy in older adults: a systematic review and meta-analysis
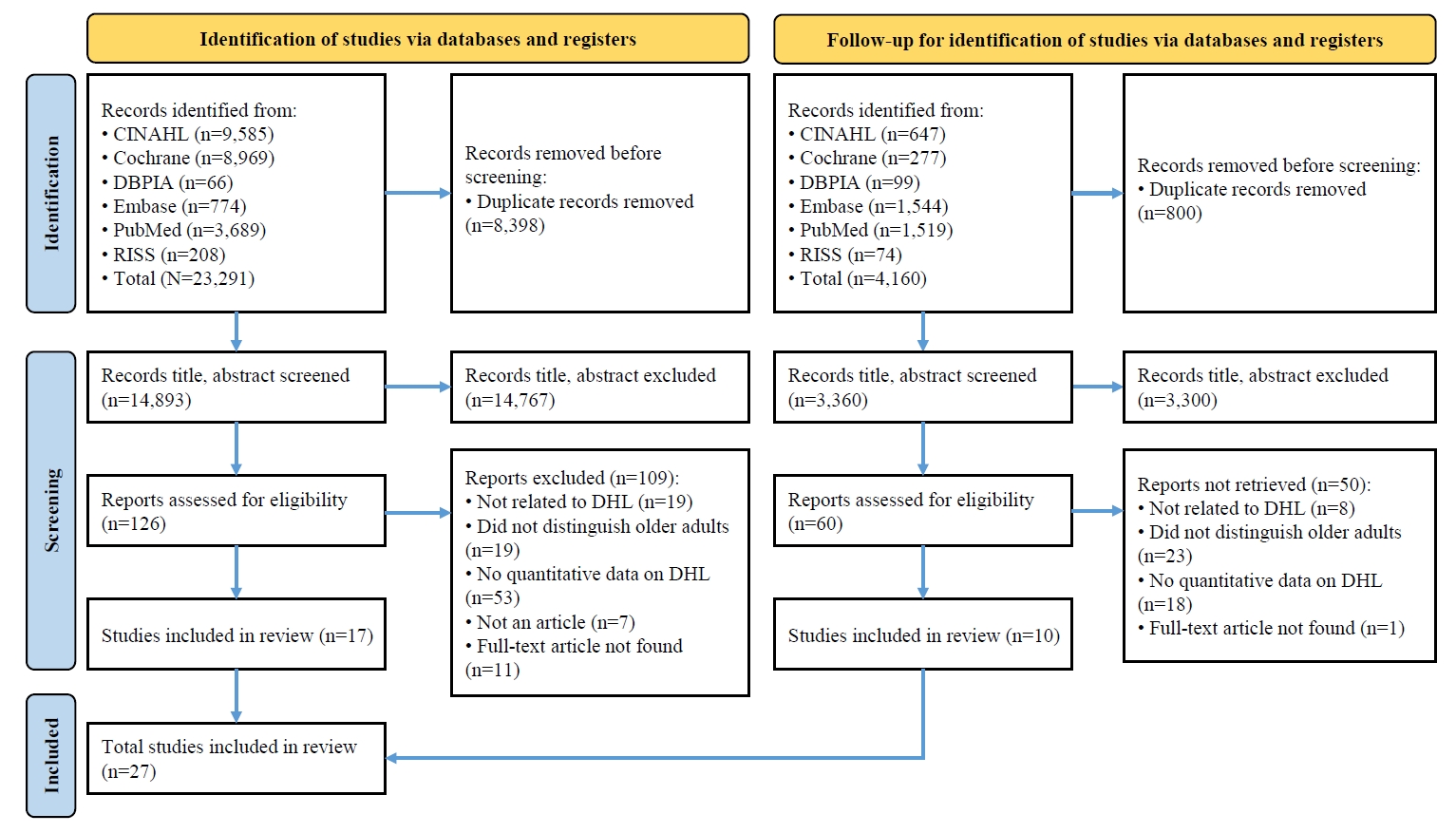
Figure 1. PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow diagram: study selection process. DHL, digital health literacy.
Figure 1.
Variables influencing digital health literacy in older adults: a systematic review and meta-analysis
| No. | Author (year) | Country | Setting | Participants | Sample size | Sampling | Age (yr) | Concept | DHL scale | DHL degree | Theory |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Chae [A1] (2024) | Korea | Community | ≥65 | 132 | Convenience | 71.6±4.73 | EHL | KeHEALS | 3.90±0.52 | No |
| 2 | Cai et al. [A2] (2024) | China | Community | ≥65 | 578 | Random | 70.1±6.13 | EHL | CeHEALS | 2.39±0.30 | No |
| 3 | Cao et al. [A3] (2023) | China | Community | ≥60 | 4,218 | Stratified and multistage | 71.9±7.2 | EHL | CeHEALS | 12.57±10.00 | No |
| 4 | Choi [A4] (2022) | Korea | Community | ≥60 | 186 | Convenience | 75.6±5.98 | EHL | KeHEALS | 28.76±6.41 | No |
| 5 | Cui et al. [A5] (2021) | China | Community | ≥60 | 1,201 | Stratified cluster | 70.1±6.29 | EHL | eHEALS | 17.24±9.34 | No |
| 6 | Dai et al. [A7] (2024) | China | Community | ≥60 | 413 | Convenience | 70.8±6.71 | EHL | eHEALS | 23.26±6.00 | IMeHU |
| 7 | Ghazi et al. [A8] (2023) | Sweden | Community | ≥65 | 490 | NR | 77.9±7.49 | EHL | eHEALS | 3.44±1.27 | No |
| 8 | Hu et al. [A6] (2023) | China | Hospital | ≥60, CD | 235 | Convenience | NR | EHL | CeHEALS | 22.11±8.59 | CMI |
| 9 | Hwang et al. [A9] (2024) | Korea | Community | ≥65, living alone | 140 | Convenience | 76.3±4.67 | DHL | DHTL-AQ | 6.64±7.46 | No |
| 10 | Hwang et al. [A10] (2025) | Korea | Community | ≥65, living alone female | 145 | Convenience | 77.5±4.83 | DHL | DHTL-AQ | 4.85±6.92 | No |
| 11 | Jiang et al. [A11] (2023) | China | Hospital | ≥65, COPD | 230 | Convenience | NR | EHL | CeHEALS | 24.66±6.86 | EHL model |
| 12 | Kim et al. [A12] (2023) | Hong Kong | Community | ≥60 | 306 | Convenience | NR | EHL | eHEALS | 3.42±0.81 | TRAM |
| 13 | Kim et al. [A13] (2023) | Korea | Community | ≥65, DM | 252 | Convenience | 72.1±5.28 | EHL | KeHEALS | 2.93±1.01 | No |
| 14 | Kim and Sung [A14] (2022) | Korea | Hospital | ≥65, cancer | 140 | Convenience | 70.8±5.33 | DHL | KeHEALS | 22.22±7.7 | No |
| 2.78±0.97 | |||||||||||
| 15 | Lee et al. [A15] (2019) | Korea | Community | 60–79, female | 203 (60s:135, 70s: 68) | Convenience | NR | EHL | eHEALS | 60s:24.31±7.99 | No |
| 70s:17.07±9.51 | |||||||||||
| 16 | Leung et al. [A16] (2022) | Hong Kong | Community | ≥60 | 266 | NR | 64.5±4.26 | DHL | DHLI | 2.83±0.46 | Salutogenesis |
| 17 | Li et al. [A17] (2020) | China | Community | ≥60 | 1,201 | Stratified cluster | 70.0±6.0 | EHL | CeHEALS | 17.24±9.34 | No |
| 2.16±1.17 | |||||||||||
| 18 | Luo et al. [A18] (2025) | China | Community | ≥60 | 1,658 | Convenience | 72.1±5.28 | EHL | CeHEALS | 23.18±6.81 | No |
| 19 | Nam and Ha [A19] (2024) | Korea | Community | ≥65, CD, living alone | 91 | Convenience | NR | EHL | KeHEALS | 24.75±7.71 | No |
| 20 | Park [A20] (2024) | USA | Community | ≥65 | 191 | Convenience | 70.9±4.30 | EHL | CeHEALS | 27.63±7.82 | No |
| 21 | Ryu and Chae [A21] (2024) | Korea | Community | ≥65 | 150 | Quota | 70.8±4.92 | EHL | KeHEALS | 31.34±4.13 | No |
| 3.92±0.52 | |||||||||||
| 22 | Son and Han [A22] (2025) | Korea | Community | ≥65 | 197 | Convenience | 71.7±5.94 | DHL | KeHEALS | 21.97±8.38 | No |
| 23 | Song and Shin [A23] (2020) | Korea | Community | ≥65 | 102 | Convenience | 70.0±4.84 | EHL | KeHEALS | 28.35±5.01 | No |
| 24 | Wang et al. [A24] (2022) | China | Community | ≥60 | 425 | Convenience | NR | EHL | eHEALS | 16.54±4.177 | KAB model and health empowerment |
| 25 | Wong et al. [A25] (2022) | Hong Kong | Community | ≥60 | 68 | NR | 71.7±6.0 | EHL | CeHEALS | 25.0±8.7 | Health empowerment |
| 26 | Wu et al. [A26] (2022) | China | Nursing home | ≥60, CD | 289 | Convenience | 68.6±5.36 | EHL | CeHEALS | 19.15±9.60 | CDSM |
| 27 | Zhu and Yang [A27] (2023) | China | Community | ≥60 | 6,183 | Convenience | 72.6±5.36 | EHL | CeHEALS | 21.17±8.25 | No |
| Category | Related variables | MA | Correlation with DHL | ||
|---|---|---|---|---|---|
| + | – | NS | |||
| Demographic | Age | O | [A7,A9,A10,A11,A14,A18,A19,A22,A23] | [A4,A8,A15] | |
| Sex (male) | O | [A8,A19,A22,A27] | [A7] | [A3,A9,A11,A14,A16,A18,A23] | |
| Physical | HRQoL | O | [A6,A27] | ||
| Cognitive function | O | [A9,A17] | [A4] | ||
| No. of chronic diseases | O | [A10,A27] | [A4] | ||
| Perceived health status | O | [A4,A7,A9,A10,A20,A23] | |||
| Sleep problem | X | [A9] | |||
| Successful aging | X | [A1] | |||
| Behavioral | Adherence of medication | X | [A19] | ||
| Continued usage intention | X | [A12] | |||
| Health-promoting behavior | O | [A5,A17,A23,A24] | [A15] | ||
| Health information-seeking behavior | X | [A4] | |||
| m-health use | X | [A13] | |||
| Self-care behavior | O | [A24,A25,A26] | [A22] | ||
| Psychosocial | Anxiety about the future | X | [A16] | ||
| Depressive symptoms | X | [A27] | |||
| Family care | X | [A6] | |||
| General self-efficacy | O | [A9,A11,A14,A18,A22,A24,A26] | |||
| Health agreeableness | X | [A6] | |||
| Health anxiety | X | [A20] | |||
| Health conscientiousness | X | [A6] | |||
| Health extraversion | X | [A6] | |||
| Health neuroticism | X | [A6] | |||
| Health openness | X | [A6] | |||
| Information satisfaction | X | [A16] | |||
| Information self⁃efficacy | X | [A8] | |||
| Innovativeness | X | [A12] | |||
| Loneliness | X | [A10] | |||
| Optimism | X | [A12] | |||
| Psychological distress | X | [A7] | |||
| Self-identity | X | [A2] | |||
| Sense of coherence | X | [A16] | |||
| Social isolation | X | [A10] | |||
| Social support | O | [A1,A11,A13,A18,A26] | [A14] | ||
| Social capital | O | [A2] | |||
| Cognitive social capital | O | [A3] | [A5] | ||
| Structure social capital | O | [A3,A5] | |||
| Technological self-efficacy | X | [A21] | |||
| Technophobia | O | [A11,A18] | |||
| Cognitive | Aging attitudes | X | [A11] | ||
| Attitude toward using DHT | X | [A12] | |||
| Digital information level | O | [A14,A21] | |||
| Educational participation motivation | X | [A2] | |||
| Health literacy | X | [A19] | |||
| Perceived eHealth importance | X | [A4] | |||
| Perceived eHealth usability | O | [A4,A12] | |||
| Perceived ease of use | X | [A12] | |||
| Perceived importance of app design | X | [A13] | |||
| Web search skills | X | [A11] | |||
| No. | Authors (year) | Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 | Total |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Chae [A1] (2024) | Y | Y | Y | Y | Y | Y | Y | Y | 8 |
| 2 | Cai et al. [A2] (2024) | Y | Y | Y | Y | Y | Y | Y | Y | 8 |
| 3 | Cao et al. [A3] (2023) | Y | Y | Y | N | Y | Y | Y | Y | 7 |
| 4 | Choi [A4] (2022) | Y | Y | N | Y | Y | Y | N | Y | 6 |
| 5 | Cui et al. [A5] (2021) | Y | Y | N | Y | Y | Y | Y | Y | 7 |
| 6 | Hu et al. [A6] (2023) | Y | Y | Y | N | Y | Y | Y | Y | 7 |
| 7 | Dai et al. [A7] (2024) | Y | Y | Y | Y | Y | Y | N | Y | 7 |
| 8 | Ghazi et al. [A8] (2023) | Y | Y | Y | Y | Y | Y | Y | Y | 8 |
| 9 | Hwang et al. [A9] (2024) | Y | Y | Y | Y | Y | Y | Y | Y | 8 |
| 10 | Hwang et al. [A10] (2025) | Y | Y | Y | Y | Y | Y | Y | Y | 8 |
| 11 | Jiang et al. [A11] (2023) | Y | Y | Y | Y | Y | Y | Y | Y | 8 |
| 12 | Kim et al. [A12] (2023) | Y | Y | Y | Y | Y | N | Y | Y | 7 |
| 13 | Kim et al. [A13] (2023) | Y | N | Y | Y | Y | Y | Y | Y | 7 |
| 14 | Kim and Sung [A14] (2022) | Y | Y | Y | N | Y | Y | Y | Y | 7 |
| 15 | Lee et al. [A15] (2019) | Y | Y | Y | Y | Y | Y | Y | Y | 8 |
| 16 | Leung et al. [A16] (2022) | Y | Y | N | Y | Y | Y | Y | Y | 7 |
| 17 | Li et al. [A17] (2020) | Y | Y | Y | Y | Y | Y | Y | Y | 8 |
| 18 | Luo et al. [A18] (2025) | Y | Y | Y | Y | Y | Y | Y | Y | 8 |
| 19 | Nam and Ha [A19] (2024) | Y | Y | Y | Y | Y | Y | Y | Y | 8 |
| 20 | Park [A20] (2024) | Y | Y | Y | Y | Y | Y | Y | Y | 8 |
| 21 | Ryu and Chae [A21] (2024) | Y | Y | Y | Y | Y | Y | Y | Y | 8 |
| 22 | Son and Han [A22] (2025) | Y | Y | Y | Y | Y | Y | Y | Y | 8 |
| 23 | Song and Shin [A23] (2020) | Y | Y | Y | Y | Y | Y | Y | Y | 8 |
| 24 | Wang et al. [A24] (2022) | Y | Y | Y | Y | Y | Y | Y | Y | 6 |
| 25 | Wong et al. [A25] (2022) | Y | Y | Y | Y | Y | N | Y | Y | 7 |
| 26 | Wu et al. [A26] (2022) | Y | Y | Y | N | Y | Y | Y | Y | 7 |
| 27 | Zhu and Yang [A27] (2023) | Y | Y | Y | Y | Y | Y | Y | Y | 8 |
| MR (%) | 100 | 94 | 100 | 88 | 100 | 94 | 100 | 100 |
| Related variables | k | ESr | 95% CI | Z | p | Homogeneity test | ||
|---|---|---|---|---|---|---|---|---|
| Q | p | I2 | ||||||
| Total overall effect size | 51 | .24 | .16 to .32 | 5.80 | <.001 | 1944.89 | <.001 | 97.4 |
| Demographic factors | 10 | .02 | –.13 to .17 | 0.25 | .802 | 83.50 | <.001 | 89.2 |
| Age | 2 | –.35 | –.68 to .11 | –1.48 | .136 | 18.70 | <.001 | 94.7 |
| Sex (male) | 8 | .10 | .02 to .18 | 2.56 | .010 | 26.30 | <.001 | 73.4 |
| Physical factors | 13 | .22 | .11 to .32 | 3.90 | <.001 | 141.47 | <.001 | 91.5 |
| HRQoL | 2 | .33 | –.04 to .62 | 1.77 | .077 | 56.97 | <.001 | 98.2 |
| Cognitive function | 3 | .28 | .18 to .36 | 5.70 | <.001 | 4.08 | .130 | 51.0 |
| No. of chronic conditions | 2 | –.15 | –.25 to –.04 | –2.68 | .007 | 0.13 | .714 | 0.0 |
| Perceived health status | 6 | .26 | .16 to .36 | 4.84 | <.001 | 18.00 | .003 | 72.2 |
| Behavioral factors | 9 | .40 | .30 to .48 | 7.50 | <.001 | 52.93 | <.001 | 84.9 |
| Health-promoting behavior | 5 | .42 | .32 to .50 | 7.87 | <.001 | 17.33 | .002 | 76.9 |
| Self-care behavior | 4 | .38 | .17 to .55 | 3.40 | .001 | 32.05 | <.001 | 90.6 |
| Psychosocial factors | 15 | .23 | .04 to .40 | 2.39 | .003 | 1168.35 | <.001 | 98.8 |
| General self-efficacy | 7 | .37 | .28 to .46 | 7.16 | <.001 | 29.48 | <.001 | 79.6 |
| Social support | 6 | .33 | .24 to .42 | 6.58 | <.001 | 21.68 | .001 | 76.9 |
| Technophobia | 2 | –.55 | –.47 to –.40 | –3.16 | .002 | 29.91 | <.001 | 96.7 |
| Cognitive factors | 4 | .50 | .33 to .64 | 5.33 | <.001 | 22.60 | <.001 | 86.5 |
| Digital information level | 2 | .62 | .55 to .69 | 12.35 | <.001 | 0.02 | .890 | 0.0 |
| Perceived eHealth usability | 2 | .37 | .29 to .44 | 8.51 | <.001 | 0.54 | .461 | 0.0 |
| Number | Search query |
|---|---|
| CINAHL: Results 1st search (n=9,585), 2nd search (n=647) | |
| #1 | (MH "Computer Literacy") OR computer literac* OR digital health literacy OR digital health OR digital literacy OR digital disparity OR digital divide OR technology literacy OR technology disparity OR technology divide OR health technology literacy OR mhealth literacy OR m-health literacy OR mobile health literacy OR mobile health education OR ehealth literacy OR e-health literacy OR electronic health literacy OR Internet literacy OR internet health literacy OR telehealth literacy OR tele-health literacy OR online literacy OR telemedicine literacy OR tele-medicine literacy OR electronic health information OR electronic health information literacy OR web based health literacy |
| #2 | (MH "Aged+") OR old* OR aged person OR aging OR senior OR ((older* OR elder* OR aged) AND people) OR ((older* OR elder*) AND adult*) |
| #3 | S1 AND S2 |
| PubMed: Results 1st search (n=3,689), 2nd search (n=1,519) | |
| #1 | "Computer Literacy"[Mesh] OR "computer literac*"[TIAB] |
| #2 | digital health literacy[TIAB] OR digital health[TIAB] OR digital literacy[TIAB] OR digital disparity[TIAB] OR digital divide[TIAB] OR technology literacy[TIAB] OR technology disparity[TIAB] OR technology divide[TIAB] OR health technology literacy[TIAB] OR mhealth literacy[TIAB] OR m-health literacy[TIAB] OR mobile health literacy[TIAB] OR mobile health education[TIAB] OR ehealth literacy[TIAB] OR e-health literacy[TIAB] OR electronic health literacy[TIAB] OR Internet literacy[TIAB] OR internet health literacy[TIAB] OR telehealth literacy[TIAB] OR tele-health literacy[TIAB] OR online literacy[TIAB] OR telemedicine literacy[TIAB] OR tele-medicine literacy[TIAB] OR electronic health information[TIAB] OR electronic health information literacy[TIAB] OR web based health literacy[TIAB] |
| #3 | "Aged"[Mesh] OR "Aged"[TIAB] OR "Elderly"[TIAB] |
| #4 | "old*"[TIAB] OR "aged person"[TIAB] OR "aging"[TIAB] OR "senior"[TIAB] OR ((older*[TIAB] OR elder*[TIAB] OR aged[TIAB]) AND people[TIAB]) OR ((older*[TIAB] OR elder*[TIAB]) AND adult*[TIAB]) |
| #5 | #1 OR #2 |
| #6 | #3 OR #4 |
| #7 | #5 AND #6 |
| Cochrane Library: Results 1st search (n=8,969), 2nd search (n=277) | |
| #1 | MeSH descriptor: [Computer Literacy] explode all trees |
| #2 | computer literac* OR ((digital OR technology OR mhealth OR m-health OR mobile OR ehealth OR e-health OR electronic OR Internet OR telehealth OR tele-health OR online OR telemedicine OR tele-medicine) NEAR/4 (literac* OR disparity OR divide)) OR mobile health education OR electronic health information OR web based health literacy |
| #3 | #1 OR #2 |
| #4 | MeSH descriptor: [Aged] explode all trees |
| #5 | old* OR aging OR senior ((ag* OR older* OR elder*) NEAR/2 (person* OR people OR adult*)) |
| #6 | #4 OR #5 |
| #7 | #3 AND #6 |
Table 1. Characteristics of studies included in systematic review and meta-analysis
Values are presented as number or mean±standard deviation unless otherwise stated. CD, chronic disease; CDSM, chronic disease self-management model; CMI, comprehensive model of information looking; COPD, chronic obstructive pulmonary disease; DHL, digital health literacy; DM, diabetes mellitus; EHL, electronic health literacy; IMeHU, integrative model of eHealth use, KAB model, knowledge, attitude, behavior model; NR, not report; TRAM, technology readiness and acceptance model.
Table 2. Classification of factors related to digital health literacy and results of studies
DHL, digital health literacy; HRQOL, health-related quality of life; MA, meta-analysis; NS, not significant; DHT, digital health technology; +, positive correlation; -, negative correlation; O, literature included in the meta-analysis; X, literature not included in the meta-analysis.
Table 3. Quality assessment of studies
Q1: Were the criteria for inclusion in the sample clearly defined?; Q2: Were the study subjects and the setting described in detail?; Q3: Was the exposure measured in a valid and reliable way?; Q4: Were objective, standard criteria used for measurement of the condition?; Q5: Were confounding factors identified?; Q6: Were strategies to deal with confounding factors stated?; Q7: Were the outcomes measured in a valid and reliable way?; Q8: Was appropriate statistical analysis used? MR, match rate; Y, yes; N, no.
Table 4. Effect size of related factors for digital health literacy of older people
CI, confidence interval; ESr, effect size; HRQoL, health related quality of life; I2, the proportion of true variance; k, number of cases; Q, Q-value between subgroups.

