 Submit an article
Submit an article
Articles
- Page Path
- HOME > J Korean Acad Nurs > Volume 53(5); 2023 > Article
- Research Paper A Caring Program for Health Promotion among Women Who Have Experienced Trauma: A QuasiExperimental Pilot Study
- Goun Kim, Heejung Kim, Jeongok Park, Hee Sun Kang, Soojin Kim, Sunah Kim
-
Journal of Korean Academy of Nursing 2023;53(5):500-513.
DOI: https://doi.org/10.4040/jkan.22120
Published online: October 31, 2023
1College of Nursing and Research Institute of Nursing Science, Pusan National University, Yangsan, Korea
2Brain Korea 21 FOUR Project, Yonsei University, Seoul, Korea
3College of Nursing and Mo-Im Kim Nursing Research Institute, Yonsei University, Seoul, Korea
4Red Cross College of Nursing, Chung-Ang University, Seoul, Korea
5College of Nursing, Chonnam National University, Gwangju, Korea
2Brain Korea 21 FOUR Project, Yonsei University, Seoul, Korea
3College of Nursing and Mo-Im Kim Nursing Research Institute, Yonsei University, Seoul, Korea
4Red Cross College of Nursing, Chung-Ang University, Seoul, Korea
5College of Nursing, Chonnam National University, Gwangju, Korea
-
Corresponding author:
Sunah Kim,
Email: psy0962@yuhs.ac
Abstract
Purpose
Women are more vulnerable to post-traumatic stress (PTS) than men, causing several health problems. Nurses should understand and work with women who have experienced trauma and provide interventions to promote their physical, social, and mental health.
Methods
This quasi-experimental pilot study used a one-group pre-test/post-test design. Data were collected from 14 women recruited between December 2019 and May 2020 from a self-sufficiency support center in South Korea for sexually-exploited women who had experienced trauma. The program consisted of six one-on-one intervention sessions per week for six weeks. Each session averaged 60~120 minutes. Participants were assessed at pre-test, post-test, and one-month follow-up. Changes in outcome variables over time were analyzed using the Wilcoxon signed-rank and Friedman tests.
Results
The caring program for health promotion was divided into six sessions: understanding the self, sharing traumatic events and negative emotions, reframing the meaning of traumatic events, identifying thoughts and physical and emotional responses, developing health promotion activities, and maintaining a positive attitude during the process of change. As a result of the caring program, PTS (F = 36.33, p < .001), depression (F = 24.45, p < .001), health-promoting behaviors (F = 7.06, p = .004), and self-esteem (F = 19.74, p < .001) among the participants differed significantly at pre-test, post-test, and follow-up.
Conclusion
This study provides foundational information for the implementation of a theory-driven program by nurses in clinical and community settings to provide comprehensive care for women who have experienced trauma.
J Korean Acad Nurs. 2023 Oct;53(5):500-513. English.
Published online Oct 31, 2023.
https://doi.org/10.4040/jkan.22120
Published online Oct 31, 2023.
https://doi.org/10.4040/jkan.22120
© 2023 Korean Society of Nursing Science
Original Article
A Caring Program for Health Promotion among Women Who Have Experienced Trauma: A Quasi-Experimental Pilot Study
Abstract
Purpose
Women are more vulnerable to post-traumatic stress (PTS) than men, causing several health problems. Nurses should understand and work with women who have experienced trauma and provide interventions to promote their physical, social, and mental health.
Methods
This quasi-experimental pilot study used a one-group pre-test/post-test design. Data were collected from 14 women recruited between December 2019 and May 2020 from a self-sufficiency support center in South Korea for sexually-exploited women who had experienced trauma. The program consisted of six one-on-one intervention sessions per week for six weeks. Each session averaged 60~120 minutes. Participants were assessed at pre-test, post-test, and one-month follow-up. Changes in outcome variables over time were analyzed using the Wilcoxon signed-rank and Friedman tests.
Results
The caring program for health promotion was divided into six sessions: understanding the self, sharing traumatic events and negative emotions, reframing the meaning of traumatic events, identifying thoughts and physical and emotional responses, developing health promotion activities, and maintaining a positive attitude during the process of change. As a result of the caring program, PTS (F = 36.33, p < .001), depression (F = 24.45, p < .001), health-promoting behaviors (F = 7.06, p =.004), and self-esteem (F = 19.74, p < .001) among the participants differed significantly at pre-test, post-test, and follow-up.
Conclusion
This study provides foundational information for the implementation of a theory-driven program by nurses in clinical and community settings to provide comprehensive care for women who have experienced trauma.
Keywords
Health Promotion; Program Development; Program Evaluation; Stress Disorders, Post-Traumatic; Women
INTRODUCTION
Trauma is an emotional response to distressing events such as serious illness, sexual assault, unexpected death of a loved one, or other violent personal assaults [1] and can cause post-traumatic stress disorder (PTSD) [2]. According to a 2013 report, 3.6% of the world’s population suffers from PTSD [3]. Traumatic events leading to PTSD are reportedly experienced by 5%~6% of men and 10%~12% of women at some point in their lives [4], thereby confirming women’s vulnerability. Women who have experienced trauma may exhibit post-traumatic stress (PTS) symptoms that make daily life difficult because of intrusive memories, avoidance, hyperarousal, negative thoughts, or mood changes associated with traumatic events [2]. They may repeatedly recall painful images related to traumatic events, have nightmares, or act or feel as if a traumatic event occurs in the present (flashback) [2].
Women with trauma experience physical, mental, and social difficulties. They are approximately 2.4 times more likely to experience mental health problems than those who have not experienced traumatic events [5]. Women who experience trauma often exhibit symptoms of depression, anxiety, low self-esteem, antisocial disorders, substance abuse (e.g., drugs and alcohol), high levels of social phobia, and high rates of attempted suicide [5, 6, 7, 8]. In addition, they can develop health conditions, such as hypertension, heart disease, diabetes, high triglyceride levels, kidney disease, digestive problems, lung disease, and back pain [9]. Therefore, it is necessary to develop an integrated health-promotion program for women who have experienced trauma.
Health promotion is the process of improving health by empowering individuals to increase their control over their health [10]. Individual health-promoting resources include sleep, breakfast, snacks, exercise, smoking cessation, drinking, and weight management [11]. A study showed that the smoking rate was 2~4 times higher, and severe obesity was 1.4~1.6 times higher in women who had experienced trauma than in those who had not [8]. In particular, if exposure to traumatic events during childhood leads to problems with health behaviors such as smoking, alcoholism, physical inactivity, severe obesity, and sleep disorders [7, 8], then interventions that can directly change health behaviors are required.
Women who have experienced trauma have a higher incidence of depression and more severe symptoms than those without trauma [12]. In particular, the higher the clinical depression score, the more trauma symptoms they show [12]. Women who have experienced trauma may also experience depression throughout their life [13, 14, 15]. Depression can lead to suicide attempts when not mediated properly [16]. Therefore, an intervention program is necessary to bring about changes in thoughts, emotions, and behavior, in addition to pharmacotherapy, to alleviate depression symptoms.
Women who have experienced trauma tend to perceive and evaluate themselves negatively, which results in low self-esteem [17]. These symptoms intensify their PTSD and inability to adapt to society [6]. Trauma survivors who exhibit avoidance behaviors tend to avoid triggering events, show hypersensitivity, lack concentration, have negative feelings about themselves and others, exhibit significantly diminished interest in important activities, and blame themselves [2]. However, trauma survivors who recognized their traumatic events from a positive and realistic perspective showed improved self-esteem as they accepted their strengths and weaknesses as they are [7, 18]. Therefore, it is necessary for survivors to integrate the series of events that have occurred to them from an objective perspective and focus on the present to discover their inner strengths.
Previous studies on women who have experienced trauma have focused on restructuring cognitive processes, reducing guilt, and teaching individuals to effectively cope with uncontrolled emotions [7, 18, 19]. In addition, exposure therapy includes integrating false information into new structures by activating fear structures and reducing PTS and depressive symptoms in women with PTSD [20]. A forgiveness program for trauma survivors provides psychological treatment to victims at risk of depression, repeated suicidal ideation, and drug or alcohol abuse [18]. However, as these women are vulnerable to physical, mental, and social health problems, an integrated intervention program is needed.
This study used Swanson’s caring theory to develop a health-promotion program for women who have experienced trauma. Swanson’s caring theory helps nurses improve the well-being of women who have experienced trauma owing to unexpected miscarriage [21]. Adolfsson [22] reported that nurses can provide appropriate professional care to help women who have experienced trauma regain their health by identifying their individual needs. This theory emphasizes that by spending time with patients and building rapport, nurses can promote their well-being by creating an environment in which patients can engage in self-care. Therefore, it is necessary to develop a comprehensive health-promotion program based on the theory that nurses can manage patients’ health problems.
1. Study aim
This study aimed to (1) develop a caring program for health promotion based on Swanson’s caring theory, for women who have experienced trauma and (2) examine its effects on PTS, depression, health-promoting behaviors, and self-esteem.
METHODS
1. Study design
This quasi-experimental pilot study used a one-group pre-test/post-test design with repeated measures to identify the effectiveness of a caring program for health promotion in women who experienced trauma. These women were evaluated at the following time points: pre-test, post-test (post-test 1, immediately after the intervention), and follow-up (post-test 2, one month after the intervention) to assess the program’s sustainability.
2. Participants
This study targeted all women participating in a self-sufficiency support center for sexually-exploited women in South Korea. Facility-based sampling was performed to recruit the hard-to-reach population [23]. The inclusion criteria were as follows: (1) women aged over 18 years who had experienced a traumatic event and (2) women with a PTS score of 64 or lower on the PTSD Checklist (PCL-5). The exclusion criteria were as follows: (1) the presence of psychiatric conditions with hallucinations and delusions and (2) a diagnosis of an intellectual disability that would make understanding the intervention procedure difficult. None of the recruited participants in this study were classified as high-risk, with a PCL-5 score exceeding 80% (64 points) of the total score.
The sample size was calculated using G*Power analysis. After calculating an effect size of 0.5, a significance level of .05, and a power of .80 with one group using a t-test, the number of estimated participants was 35. As an appropriate sample size was not reached, data were analyzed using a non-parametric test.
Seventeen sexually-exploited women affiliated with the center agreed to participate in the study. Of these, three dropped out before post-test 1, resulting in 14 participants completing the interventions and surveys. Of the three women who dropped out, two moved to another region, and one refused to continue the program. Therefore, data from the remaining 14 participants were analyzed. The participants did not receive additional training at the center of the program to control for the diffusion effect.
3. Measurements
1) Post-traumatic stress
PTS was measured using the PCL-5, which was developed by Weathers et al. [24] and revised by Weathers et al. [25] according to the revised PTSD definition in the Diagnostic and Statistical Manual of Mental Disorders-5 (DSM-5) and translated into Korean by Kim et al. [26]. The Korean version of the PCL-5 (PCL-5-K) comprises 20 items, each scored from 0 (not at all) to 4 (extremely high). The score indicates the severity of symptoms caused by stress-related traumatic events during the last month. Possible scores range from 0 to 80, with higher scores indicating more severe PTSD symptoms [26]. Cronbach’s alpha for the PCL-5-K was .97 among Korean veterans of the Vietnam War [26] and .89 in this study.
2) Depression
Depression was assessed using the Center for Epidemiologic Studies Depression Scale (CES-D) developed by Radloff [27] and translated into Korean by Chon & Rhee [28]. The Korean version of the CES-D comprises 20 items rated on a 4-point Likert scale (0 = rarely or none of the time, 1 = some or a little of the time, 2 = occasionally or a moderate amount of the time, 3 = most or all of the time) according to how respondents felt during the last week. Possible scores range from 0 to 60, with higher scores indicating higher levels of depression [27]. Cronbach’s alpha for the Korean CES-D was .89 among Korean adults [28] and .78 in this study.
3) Health-promoting behaviors
Health-promoting behaviors were measured using the Health Promoting Lifestyle Profile-II (HPLP-II) developed by Walker et al. [29] and translated into Korean by Yun & Kim [30]. The Korean version of the HPLP-II comprises 52 items rated on a 4-point Likert scale (1 = never, 2 = sometimes, 3 = often, and 4 = routinely). Possible scores ranged from 52 to 208, with higher scores indicating higher levels of health-promoting behaviors. Cronbach’s alpha for the Korean HPLP-II was .91 among Korean adult women [30] and .92 in this study.
4) Self-esteem
Self-esteem was assessed using the Rosenberg Self-Esteem Scale (RSES) developed by Rosenberg [31] and translated into Korean by Bae et al. [32]. The Korean version of the RSES (K-RSES) comprises 10 items rated on a 4-point Likert scale (1 = strongly disagree, 2 = disagree, 3 = agree, and 4 = strongly agree). Possible scores range from 10 to 40, with higher scores indicating higher self-esteem. Cronbach’s alpha for the K-RSES was .90 among Korean adults [32] and in this study.
5) General and clinical characteristics
General and clinical characteristics included age, religion, marital status, education, employment, monthly income, exercise, medication, and physical disease. Smoking status was assigned as either “past smoker or nonsmoker” or “current smoker.” Drinking status was assigned as either “past drinker or nondrinker” or “current drinker.”
4. Caring program for health promotion
1) Development process
The caring program development process is as follows: First, needs assessment interviews were conducted with stakeholders at the self-sufficiency support center. The stakeholders included two activists who understood the purpose of the study and provided written informed consent before the interviews. Each had more than ten years of practical experience working with women who had experienced trauma, had a well-developed understanding of the needs of women who had experienced sexual trauma, and could confidently communicate their opinions. After analyzing the content of the interviews, six themes concerning the needs of women who had experienced trauma emerged: (1) self-understanding, (2) negative emotion conversion, (3) self-esteem improvement, (4) irregular sleep habit improvement, (5) somatic symptom control, and (6) health-promoting activities. These needs were considered during the development of the program.
Second, the program type and method were determined based on a literature review. Both individual and group interventions have been used for women who have experienced trauma, particularly those with PTS. In the context of group interventions, it can be difficult for women to disclose wounds caused by various traumatic events in front of multiple group participants. Individual interventions have the advantage in that participants can proceed at their own pace without being influenced by the progress of others. As each individual experiences different degrees of PTS, this approach allows for adjustment of the time and duration of the intervention according to symptom severity [18]. This program was structured according to recommendations in the literature as a one-on-one intervention conducted over six sessions [7, 18], with each session lasting between 60 and 120 minutes [18].
Finally, the outline, protocol, and worksheets of the initially developed program were reviewed and modified by experts, including six nurses employed at mental health centers, one mental health professor, and two stakeholders from the support center. The evaluation resulted in an average of 3.5 points on a 4-point Likert scale (1 = not at all appropriate, 2 = not appropriate, 3 = appropriate, and 4 = very appropriate) and a content validity index of 83.3%, indicating a high degree of validity and appropriateness. Expert feedback was used to modify the program. Modifications were made to (1) make the terms in the worksheet easier to understand; (2) include additional content on drug use, drinking, and smoking risks; (3) provide activities rather than explanations to enhance participants’ interest and concentration; (4) provide homework for each session to maintain continuity between sessions; (5) include music to stimulate the autonomic nervous system at the beginning and end of each session and during breathing meditation; and (6) provide space and time for participants to remember three pleasurable or happy experiences during the weekly session.
2) Caring program for health promotion
The caring program consisted of six individual intervention sessions per week for six weeks. Each session averaged 60~120 minutes. All sessions began with muscle relaxation activities with relaxing background music. The participants shared three experiences for which they were grateful. Each session provided homework assignments with content that could be applied in daily life or used to organize thoughts.
This study used Swanson’s caring theory to develop a health promotion program for women who have experienced trauma (Figure 1). Swanson’s caring theory outlines five caring processes: maintaining beliefs, knowing, being with, doing for, and enabling [21]. This program included the following concepts: understanding the self, sharing traumatic events and negative emotions, reframing the meaning of traumatic events, identifying thoughts and physical and emotional responses, developing health-promoting activities, and maintaining a positive attitude during the process of change (Table 1).
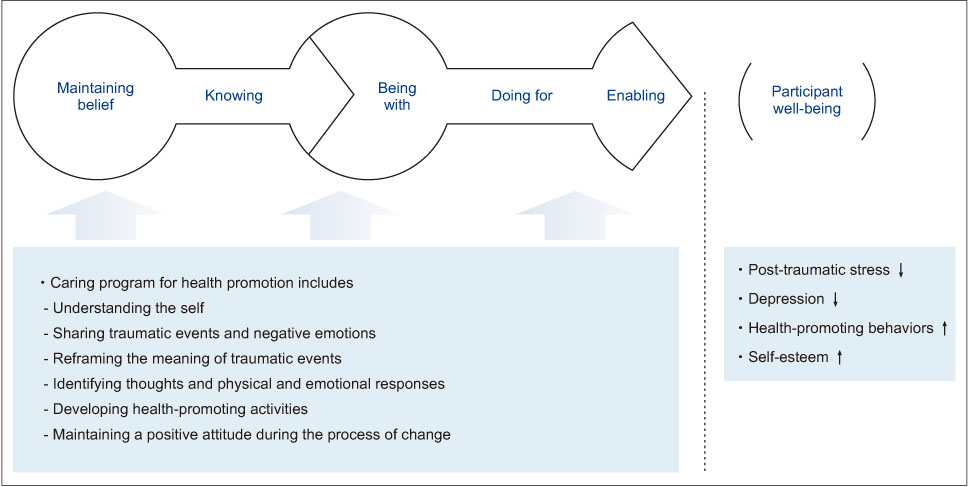
Figure 1
Conceptual framework used in this study based on Swanson’s caring theory.
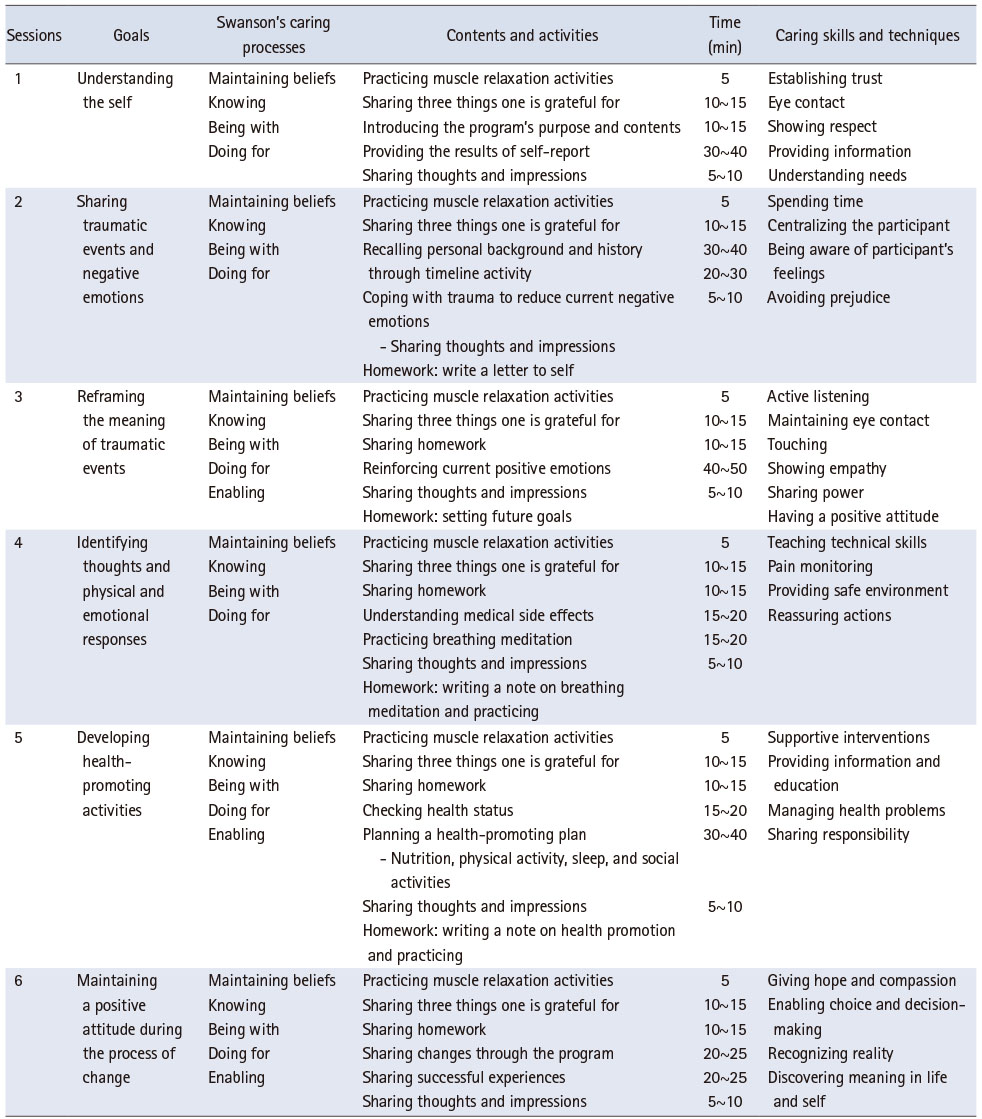
Table 1
Outline of the Caring Program for Health Promotion in Women Who Have Experienced Trauma
First, in the “maintaining beliefs” stage, trust between the participant and nurse is essential [21]. Women who have experienced trauma may incorrectly recall events. These responses may cause discomfort [33]. However, trauma survivors experience relief in knowing that a diagnosis exists and that although they are psychologically or spiritually wounded, they can heal [34]. Swanson emphasized that nurses should help patients maintain self-esteem and hope while remaining respectful [21]. Session 1 focused on understanding oneself. The participants received detailed guidance on the purpose and content of the program to help them recognize the significance of their trauma. Additionally, Session 1 emphasized the autonomy of participation in the program and specified the necessary rules that would be followed as the program progressed. Participants took time to understand themselves by monitoring their current status, which was assessed using questionnaires on PTS, depression, health-promoting behaviors, and self-esteem. The researcher focused on women who had experienced trauma and physical and mental health problems consequent to the trauma. The researcher shared their status of PTS, depression, health-promoting behaviors, and self-esteem.
Second, in the “knowing” stage, the nurse attempts to understand the meaning of an event in the participant’s life [21]. Traumatic events can negatively affect maintenance of emotional control [35]. However, this is a natural reaction, and trauma survivors require time to learn how to manage previous traumatic events [34]. Swanson indicated that nurses should avoid making assumptions about participants and should focus on their care [21]. In this study, Session 2 focused on sharing traumatic events and negative emotions. The participants recalled their personal background and history by drawing a timeline from birth to the present. They addressed traumatic events on a timeline by focusing on facts, names, and other information. When a participant recalled a traumatic event, relaxation therapy was administered to stop or reduce PTS symptoms such as intrusive memories, avoidance, hyperarousal, flashbacks, and negative changes in thought and mood [2]. Session 2 emphasized the ways to identify and cope with negative emotions arising from traumatic events. The participants then wrote a letter to themselves (by writing or drawing), and as homework, they gave themselves a small gift (doll, pencil, or hairpin). The researcher focused on avoiding prejudice, spending time with the participants, and paying close attention to them. The goal was to find clues regarding things that could cause problems, carefully analyze them, comprehend their experiences and emotions, and attentively listen to and understand their verbal and nonverbal expressions, such as eye contact and body language. The researcher communicated awareness of physical, mental, social, and cultural effects by considering traumatic events from a new perspective.
Third, in the “being with” stage, nurses shared meaning, feelings, and experiences with the participants to communicate their emotional presence [21]. Trauma survivors may react sensitively, experience amplified fear, and experience pain when faced with triggering events that they have previously avoided revisiting [34]. Swanson stressed that nurses should communicate clearly with participants and not overburden them [21]. In this study, Session 3 highlighted the reframing of the meaning of traumatic events. Participants identified their strengths and weaknesses and considered their shortcomings from different perspectives. This led them to examine trauma from different perspectives. Session 3 provided methods for creating and strengthening positive emotions. Participants focused on the present, and their feelings of stability were evaluated. In addition, participants shared what they felt grateful for. They focused on themselves by focusing on their inner selves. They use their strengths to formulate future goals for internal growth. The researcher actively listened to the participants with a positive attitude and provided feedback to ensure a clear understanding of what was being said, while showing empathy and compassion. They discussed participants’ strengths and emphasized that trauma was not a participant’s fault, with an empathetic attitude and without criticism.
Fourth, in the “doing for” stage, nurses provide care to participants [21]. Women who have experienced trauma may worry or feel nervous about everything or may have recurrent intrusive memories, which can lead to physical changes such as increased muscle tension, blood pressure, and nausea [2]. The fourth stage identified thoughts and physical and emotional responses elicited. Swanson emphasized that nurses should help participants maintain their well-being by protecting and caring for them and enabling them to set their own goals [21]. This formed the focus of Session 4 of this study. The participants identified the physical symptoms they experienced when recalling their traumatic events. They practiced breathing meditation to control physical symptoms by relaxing with music and sharing thoughts, feelings, emotions, and specific physical sensations [36]. The participants were also informed about the potential side effects and the caution required when taking psychiatric drugs. The researcher provided a safe environment for objective examination of the participants’ traumatic events through breathing meditation.
Fifth, in the “enabling” stage, nurses enable participants to change their daily lives and solve problems on their own when they encounter new events [21]. In this study, Session 5 focused on developing health-promoting activities. The following health-promoting behaviors were explained: proper eating and sleeping habits and physical and social activities. Additionally, participants examined their current nutrition, sleep, and physical and social activity practices. While sharing their health behaviors, participants set specific goals by selecting the health behaviors that needed to be changed. Swanson emphasizes that nurses should provide participants with new information and support [21]. The researcher recognized participants’ anticipated needs, proposed alternatives for problem solving, received feedback, and assisted in developing a plan for health-promoting activities.
Finally, in the “well-being” stage, nurses should promote participant’s well-being by helping them recognize reality and facilitate activities while being together physically and emotionally and maintaining basic human trust [21]. By increasing their inner strength during the recovery process, trauma survivors can develop a more positive self-image, engage in meaningful activities, focus on a new life, and embrace their vulnerable selves [37]. In this study, Session 6 emphasized the maintenance of a positive attitude during the process of change. Participants shared their actions to change their health behaviors and feelings. They identified other strengths that they possessed but had never been previously recognized. This session focused on how to control emotions and maintain the previously identified health-promoting activities by applying these strengths. The researcher assisted the participants in discovering changes in their lives and in providing health guidance.
5. Data collection and procedure
Data were collected at a self-sufficiency support center for sexually-exploited women in Gwangju, South Korea. This center is a place where sexually-exploited women can visit during the day for vocational rehabilitation, employment information, and training at a related institution to help them find jobs. The users of the center are women who have been sexually exploited outside school since adolescence and have received social integration training for up to three years. First, the researcher asked whether it would be possible to conduct this study at a center with the support center director, as this population was difficult to reach. The director verified participants’ interests and intentions to participate and approved the study.
Data were collected between December 2019 and May 2020. The pre-test consisted of a structured questionnaire containing questions on general and clinical characteristics, PTS, depression, health-promoting behaviors, and self-esteem. It was administered during orientation prior to the start of the program. The post-test 1 survey was conducted using a structured questionnaire immediately after the program ended. Post-test 2 was conducted as a follow-up one month after completing the program. Both the post-test 1 and 2 contained only questions on PTS, depression, health-promoting behaviors, and self-esteem. All questionnaires were created using Google Forms, an online survey format accessible through a smartphone via text message.
The researcher is a registered woman nurse with experience in locked and open wards in psychiatric hospitals for more than four years, holds a master’s degree in psychological nursing, and is a certified psychiatric and mental health nurse. All sessions were conducted by one researcher. The stakeholders did not participate in the program and only provided a place for the researcher to proceed independently.
6. Data analysis
Statistical analyses were conducted using SPSS software 27.0 (IBM Corp., Armonk, NY, USA). Descriptive statistics were calculated for general and clinical characteristics, PTS, depression, health-promoting behaviors, and self-esteem. To accommodate the small sample size, non-parametric tests (Wilcoxon signed-rank and Friedman tests) were used to test the differences at different time points. All statistical tests were two-tailed, and statistical significance was set at p < 0.05.
7. Ethical consideration
This study was approved by the Institutional Review Board (IRB) from Yonsei University (IRB No. Y-2019-0153). This study was registered at the clinical trials data bank (https://clinicaltrials.gov/)—U.S. National Library of Medicine (clinical trial registration number: NCT05118438; last verified in November, 2021)—and is available online.
The researcher explained the procedures and objectives, expected outcomes and risks, confidentiality, compensation methods, and the participants’ right to withdraw at any time without penalty. Additionally, the participants were given time to ask questions at the end of the explanation. If any questions arose, the researcher responded immediately. Participants who wished to participate were provided with an in-depth explanation, a description of the research, and a written consent form to ensure complete comprehension. Thereafter, they were informed that they could discuss the issue with their family and acquaintances before finalizing their decision about participation. They were given time to make the decision. Consent was obtained from a private counseling room.
After obtaining written consent, the researcher selected participants who met the inclusion criteria and stayed at the center. Participants underwent a PTS assessment using a Google Form accessible on a smartphone, and only those with a score of 64 or less were enrolled in the program. A pre-test was conducted among participants who met the selection criteria, and interventions were provided. Written consent forms were stored in a locked cabinet in the researcher’s office. The participants’ responses were stored and managed on a computer that was only accessible to the researcher. The file was also encrypted for document and data management security. The collected questionnaires will be destroyed after three years, according to the IRB guidelines.
The researcher conducted the program in a designated room to protect participants’ confidentiality. If the participants felt anxious during the intervention, the researcher was prepared to measure their anxiety, using the Visual Analogue Scale-Anxiety (VAS-A) to assess its degree [38]. This tool uses a 10 cm vertical line ranging from 0 (no anxiety) to 10 (highest anxiety level), with higher scores indicating higher levels of anxiety. Participants with a VAS-A score of seven or more will be withdrawn from the program and assisted in implementing stabilization techniques. In this study, none of the participants interrupted the program because of high levels of anxiety. The participants were provided with monetary gifts after the surveys and sessions.
RESULTS
1. General and clinical characteristics
Table 2 presents the general characteristics of the 14 participants who completed all interventions and surveys. All participants were in their 20s (71.9%) and 30s (28.1%). All worked for less than 40 hours a week through work and internship programs at the self-sufficiency support center. Their average monthly income was less than US $820. Although 42.9% of the participants were high school graduates, they had passed a qualification exam equivalent to a high school diploma. Most participants were current smokers (85.7%) or drinkers (85.7%). Approximately 83.3% of smokers reported smoking one pack of cigarettes or more daily, whereas almost all drinkers reported drinking three or more times a week with one to six bottles or cans per occasion.
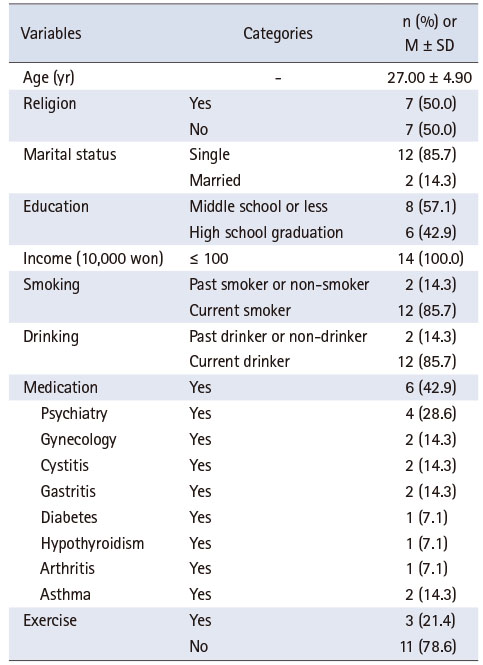
Table 2
General and Clinical Characteristics of the Participants (N = 14)
Participants have experienced the following types of traumatic events: sexual violence, which is the most common type of traumatic event, including rape; sexual acts through force or threat of harm; unwanted sexual experiences by a sibling or someone else; and verbal or physical aggression, including beating and kicking by a family member, romantic partner, or someone else. In addition, there have been cases of suicide, death of a family member, imprisonment, and life-threatening illnesses. The mean PTS score at the pre-test was 43.93 (score range: 0~80).
2. Effects of the caring program
Table 3 presents the changes in the outcomes over time. There were statistically significant differences in the scores for PTS (F = 36.33, p < .001), depression (F = 24.45, p < .001), health-promoting behaviors (F = 7.06, p = .004), and self-esteem (F = 19.74, p < .001) over the course of the caring program for health-promotion in women who experienced trauma at pre-test, post-test 1, and post-test 2.
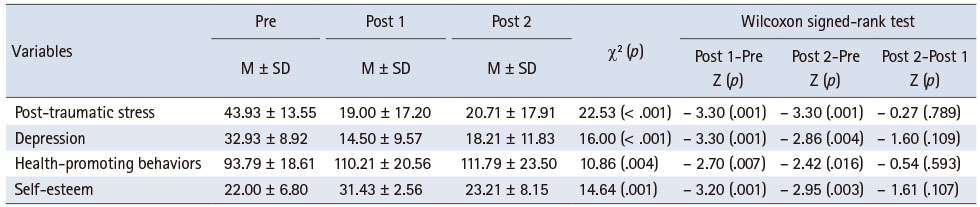
Table 3
Effects of a Caring Program for Health Promotion (N = 14)
There were statistically significant differences in the PTS, depression, health-promoting behaviors, and self-esteem scores before and after the nursing intervention. There were significant differences in PTS (Z = -3.30, p = .001), depression (Z = -3.30, p = .001), health-promoting behaviors (Z = -2.70, p = .007), and self-esteem (Z = -3.20, p = .001) scores between the pre-test and post-test 1. Regarding the scores at pre-test and post-test 2, PTS (Z = -3.30, p = .001), depression (Z = -2.86, p = .004), health-promoting behaviors (Z = -2.42, p = .016), and self-esteem (Z = -2.95, p = .003) showed statistically significant differences.
DISCUSSION
Based on Swanson’s caring theory [21], this study developed a caring program for health promotion in women who had experienced trauma and evaluated its effectiveness. Statistically significant improvements were observed in PTS, depression, health-promoting behaviors, and self-esteem from pre-test to post-test 1 and post-test 2 in all participants.
The caring program was designed to facilitate integrated health promotion among women who experienced trauma. Identifying changes in health promotion affects the maintenance and promotion of an individual’s physical and mental well-being [39]. In addition, the program enabled the researcher to become acquainted with the participants, encourage them to realize their potential, and build trust with them based on Swanson’s caring theory [21]. A face-to-face method was used on an individual basis [40, 41] in a quiet and private space where only the researcher and participants were present, which allowed rapport building. The individualized intervention used in this study was effective, considering that the participants were women who had experienced trauma. The researcher was able to provide interventions that aligned with individual symptoms. Participants practiced adjusting to negative emotions as they focused on their lives and explored themselves during the traumatic event [7]. Subsequently, the participants had the opportunity to restructure their cognitive processes by objectively examining traumatic events and focusing on their current lives.
PTS decreased more significantly at post-test 1 and post-test 2 than at pre-test. The average PTS score was 43.9 points at pre-test, with a cutoff score of 37 points or more indicating PTSD, confirming the severity of PTS. Compared to the average score of Korean veterans of the Vietnam War suffering from PTSD (47.6 points), as measured by the PCL-5 [26], participants in this study scored an average of 49.2 points, indicating a high risk of PTSD. Through this program, the participants were encouraged to reconstruct the meaning of traumatic events by examining them from different perspectives. In addition, the participants participated in the process of integrating previous events while sequentially recalling all events in their lives, both positive and traumatic. They practiced self-regulation through abdominal breathing to reduce their physical symptoms. Therefore, an individualized approach to identify the fundamental source of pain may help alleviate PTS [40, 41, 42]. Following Swanson’s theory of caring, nurses should provide tailored care that offers comfort and emphasizes reality, while sharing their feelings with those who experience these symptoms [21].
Depression significantly decreased at post-test 1 and post-test 2, as than at the pre-test. Depression caused by traumatic events can last for a lifetime [13, 15]. The average CES-D depression score at pre-test in this study (32.93) was higher than that of Korean adults with suicidal ideation (17.6) [16], highlighting the severity of their depression. After participating in the caring program, depression scores at post-test 1 decreased to 14.5, confirming the effectiveness and necessity of the intervention. However, some participants used psychiatric medications for depression. They reported that their lives were lonely, difficult, and frustrating. If depression is not properly addressed, it can lead to suicide attempts [43]. Moreover, 64.2% of the participants in this study had attempted suicide several times. Future studies should include psychiatric drug education that considers the medications that the participants are taking.
Health-promoting behaviors at pre-test, post-test 1, and post-test 2 showed statistically significant differences. After a traumatic event, survivors may engage in poor health behaviors such as physical inactivity, non-adherence to medication, and smoking [44]. Women who experience trauma are also more likely to develop various health issues, including heart, lung, and liver diseases [8]. At pre-test, the average health-promoting behavior score was 93.79 points, which was significantly lower than that of Korean adults working in an office setting (127.11 points) [45]. In addition, 42.9% of the participants were taking medications for physical illnesses, and most (85.7%) were vulnerable to physical health issues owing to their smoking and drinking habits. Participants learned how to monitor their health behaviors and developed and implemented plans to promote their health. Therefore, to improve health-promoting behaviors in women who have experienced trauma, it is necessary to provide integrated interventions that consider both physical and psychological aspects. Most importantly, nurses should provide individualized, patient-centered, and integrated interventions according to patients’ health status, emotional changes, nutritional conditions, and physical symptoms according to the disease [46].
Self-esteem showed a statistically significant difference between pre-test, post-test 1, and post-test 2. Women who have experienced trauma may have low self-esteem because of anger, shame, and guilt [18]. The participants’ average score at pre-test was lower than that of the general Korean adult population (32.8) [32]. Because women who have experienced trauma have low self-esteem and often experience difficulties establishing relationships with others [6, 7], providing accurate information about their condition is a prerequisite. Participants experienced a process for understanding themselves through this program, and the subsequent modification of their self-image could help increase their self-esteem [7]. However, participants should continue their efforts to develop a positive image of their strengths and successes even after the program [7]. In this study, self-esteem scores decreased to near pre-test levels at the one-month follow-up. This confirms that after the program ended, some participants did not actively work on maintaining their self-esteem, such as finding gratitude in their daily lives or making efforts to think positively. In future programs, it is recommended to provide homework for participants to write down what they are grateful for in a notebook daily to maintain a habit of positive thinking.
This study has several limitations. First, the sample size is small. At least 20~25 participants per group are required for the effect size to be moderate or high [47]. Although it is difficult to recruit participants because of limited access to appropriate candidates, future studies should increase the number of participants to measure the effect size. Second, this study was conducted in a single group and did not include a control group. Although we attempted to minimize the diffusion effect by ensuring that participants did not participate in any educational activities other than vocational training events outside the program, vocational training events might have affected the post-survey responses, which in turn might have affected the results. The same survey conducted at three time points might have caused a testing effect, and any unexpected event could have produced maturation effects [48]. Therefore, an experimental study with a control group should be conducted to confirm the effects of the program. Third, the results of the study are difficult to generalize. Participant recruitment was limited to women using a self-sufficiency support center for sexually exploited women in Korea. Overall, the number and diversity of participants were insufficient, which might have introduced selection bias [47] and blinding. The center where this study was conducted was part of a national organization; therefore, other institutions could be included to increase diversity.
CONCLUSION
This study developed a health-promotion caring program for women who have experienced trauma based on Swanson’s theory of caring, a patient-centered theoretical framework. The caring program provides an environment in which the health of women who have experienced trauma can be fostered through comprehensive evaluation and interpretation. This experience allowed nurses to understand participants’ past, present, and future perspectives and identify the caring behaviors required to assist them. The findings of this study indicate that the program has positive effects on PTS, depression, health-promoting behaviors, and self-esteem in women who have experienced trauma. Such programs can enhance the mental and physical health of sexually-exploited women, particularly in the context of self-sufficient support centers.
Notes
CONFLICTS OF INTEREST:Park, Jeongok and Kang, Hee Sun have been the editorial board members of JKAN since 2022 but has no role in the review process. Except for that, no potential conflict of interest relevant to this article was reported.
FUNDING:This research was supported by Mo-Im Kim Nursing Research Institute and Yonsei University College of Nursing and the National Research Foundation of Korea (NRF) grant funded by the Korean government (NRF-2018R1A2B600 1504 and 2021R1I1A1A01056240).
AUTHOR CONTRIBUTIONS:
Conceptualization or/and Methodology: Kim G & Kim H & Park J & Kang HS & Kim SJ & Kim SA.
Data curation or/and Analysis: Kim G & Kim SA.
Funding acquisition: Kim G & Kim SA.
Investigation: Kim G.
Project administration or/and Supervision: Kim H & Park J & Kang HS & Kim SJ & Kim SA.
Resources or/and Software: Kim G & Kim H & Park J & Kang HS & Kim SJ & Kim SA.
Validation: Kim G & Kim H & Park J & Kang HS & Kim SJ & Kim SA.
Visualization: Kim G & Kim H & Park J & Kang HS & Kim SJ & Kim SA.
Writing original draft or/and Review & Editing: Kim G & Kim H & Park J & Kang HS & Kim SJ & Kim SA.
ACKNOWLEDGMENTS
We acknowledge the support of Dr. Kijun Song at the Mo-Im Kim Nursing Research Institute and Yonsei University College of Nursing for reviewing and interpreting our data.
DATA SHARING STATEMENT
Please contact the corresponding author for data availability.
References
-
Kessler RC, Aguilar-Gaxiola S, Alonso J, Benjet C, Bromet EJ, Cardoso G, et al. Trauma and PTSD in the WHO world mental health surveys. European Journal of Psychotraumatology 2017;8 Suppl 5:1353383 [doi: 10.1080/20008198.2017.1353383]
-
-
American Psychiatric Association (APA). Diagnostic and statistical manual of mental disorders: DSM-5. 5th ed. Washington, DC: American Psychiatric Association Publishing; 2013. pp. 289-299.
-
-
World Health Organization (WHO). WHO releases guidance on mental health care after trauma [Internet]. Geneva: WHO; c2013 [cited 2022 Apr 10].Available from: https://www.who.int/news/item/06-
08- 2013- who- releases- guidance- on- mental- health- care- after- traum .
-
-
Olff M. Sex and gender differences in post-traumatic stress disorder: An update. European Journal of Psychotraumatology 2017;8 Suppl 4:1351204. [doi: 10.1080/20008198.2017.1351204]
-
-
Fergusson DM, Boden JM, Horwood LJ. Exposure to childhood sexual and physical abuse and adjustment in early adulthood. Child Abuse & Neglect 2008;32(6):607–619. [doi: 10.1016/j.chiabu.2006.12.018]
-
-
Jung K, Steil R. A randomized controlled trial on cognitive restructuring and imagery modification to reduce the feeling of being contaminated in adult survivors of childhood sexual abuse suffering from post-traumatic stress disorder. Psychotherapy and Psychosomatics 2013;82(4):213–220. [doi: 10.1159/000348450]
-
-
Felitti VJ, Anda RF, Nordenberg D, Williamson DF, Spitz AM, Edwards V, et al. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults. The Adverse Childhood Experiences (ACE) study. American Journal of Preventive Medicine 1998;14(4):245–258. [doi: 10.1016/s0749-3797(98)00017-8]
-
-
Farhood L, Dimassi H, Strauss NL. Understanding post-conflict mental health: Assessment of PTSD, depression, general health and life events in civilian population one year after the 2006 war in South Lebanon. Journal of Traumatic Stress Disorders and Treatment 2013;2(2):1000103 [doi: 10.4172/2324-8947.1000103]
-
-
World Health Organization (WHO). Ottawa charter for health promotion [Internet]. Geneva: WHO; [cited 2022 Apr 6].Available from: http://www.who.int/healthpromotion/conferences/previous/ottawa/en/ .
-
-
Meshberg-Cohen S, Presseau C, Thacker LR, Hefner K, Svikis D. Posttraumatic stress disorder, health problems, and depression among African American women in residential substance use treatment. Journal of Women’s Health 2016;25(7):729–737. [doi: 10.1089/jwh.2015.5328]
-
-
Lindert J, von Ehrenstein OS, Grashow R, Gal G, Braehler E, Weisskopf MG. Sexual and physical abuse in childhood is associated with depression and anxiety over the life course: Systematic review and meta-analysis. International Journal of Public Health 2014;59(2):359–372. [doi: 10.1007/s00038-013-0519-5]
-
-
Adolfsson A. The EKC-model provides empathy, knowledge and care for women that encounter health issues during the reproductive life. International Journal of Gynecology & Clinical Practices 2016;3:121 [doi: 10.15344/2394-4986/2016/121]
-
-
Shaghaghi A, Bhopal RS, Sheikh A. Approaches to recruiting‘hard-to-reach’ populations into research: A review of the literature. Health Promotion Perspectives 2011;1(2):86–94. [doi: 10.5681/hpp.2011.009]
-
-
Weathers FW, Litz BT, Herman DS, Huska JA, Keane TM. The PTSD checklist (PCL): Reliability, validity, and diagnostic utility; Poster session presented at: Annual Convention of the International Society for Traumatic Stress Studies; 1993 Oct; San Antonio, TX.
-
-
Weathers FW, Litz BT, Keane TM, Palmieri PA, Marx BP, Schnurr PP. The PTSD checklist for DSM-5 (PCL-5) [Internet]. White River Junction: National Center for PTSD; c2013 [cited 2021 Apr 3].
-
-
Kim JW, Chung HG, Choi JH, So HS, Kang SH, Kim DS, et al. Psychometric properties of the Korean version of the PTSD Checklist-5 in elderly Korean veterans of the Vietnam war. Anxiety and Mood 2017;13(2):123–131. [doi: 10.24986/anxmod.2017.13.2.010]
-
-
Radloff LS. The CES-D scale: A self-report depression scale for research in the general population. Applied Psychological Measurement 1977;1(3):385–401. [doi: 10.1177/014662167700100306]
-
-
Chon KK, Rhee MK. Preliminary development of Korean version of CES-D. Korean Journal of Clinical Psychology 1992;11(1):65–76.
-
-
Walker SN, Sechrist KR, Pender NJ. The health promoting lifestyle profile II [Internet]. Omaha: University of Nebraska Medical Center; c1995 [cited 2022 Apr 10].
-
-
Yun SN, Kim JH. Health-promoting behaviors of the women workers at the manufacturing industry-based on the Pender’s Health Promotion Model. Korean Journal of Occupational Health Nursing 1999;8(2):130–140.
-
-
Rosenberg M. In: Society and the adolescent self-image. Princeton (NJ): Princeton University Press; 1965. pp. 338.
-
-
Bae HN, Choi SW, Yu JC, Lee JS, Choi KS. Reliability and validity of the Korean version of the Rosenberg Self-Esteem Scale(K-RSES) in adult. Journal of Korean Society for Depressive and Bipolar Disorders 2014;12(1):43–49.
-
-
Metcalfe J, Jacobs WJ. A “hot-system/cool-system” view of memory under stress. PTSD Research Quarterly 1996;7(2):1–3.
-
-
Schauer M, Neuner F, Elbert T. In: Narrative exposure therapy: A short-term treatment for traumatic stress disorders. 2nd rev. and expand. ed. Cambridge (MA): Hogrefe Publishing; 2011. pp. 59-72.
-
-
Seppälä EM, Nitschke JB, Tudorascu DL, Hayes A, Goldstein MR, Nguyen DT, et al. Breathing-based meditation decreases post-traumatic stress disorder symptoms in U.S. military veterans: A randomized controlled longitudinal study. Journal of Traumatic Stress 2014;27(4):397–405. [doi: 10.1002/jts.21936]
-
-
Vogelsang J. The visual analog scale: An accurate and sensitive method for self-reporting preoperative anxiety. Journal of Post Anesthesia Nursing 1988;3(4):235–239.
-
-
Blake VK, Nehrkorn AM, Patrick JH. Differential effects of health-promoting behaviors on wellbeing among adults. International Journal of Wellbeing 2017;7(2):28–42. [doi: 10.5502/ijw.v7i1.471]
-
-
Bang KS, Lee IS, Kim SJ, Song MK, Park SE. The effects of urban forest-walking program on health promotion behavior, physical health, depression, and quality of life: A randomized controlled trial of office-workers. Journal of Korean Academy of Nursing 2016;46(1):140–148. [doi: 10.4040/jkan.2016.46.1.140]
-
-
Jiang M, Li T, Huang L, Zhuang Y. Effect of a comprehensive nursing care on the treatment of ulcerative keratitis and patient’s emotions. International Journal of Clinical and Experimental Medicine 2018;11(11):12676–12681.
-
-
Marsden E, Torgerson CJ. Single group, pre- and post-test research designs: Some methodological concerns. Oxford Review of Education 2012;38(5):583–616. [doi: 10.1080/03054985.2012.731208]
-
 Cite
Cite
