 Submit an article
Submit an article
Articles
- Page Path
- HOME > J Korean Acad Nurs > Volume 47(5); 2017 > Article
- Original Article Effects of Bullying Experience on Psychological Well-Being Mediated by Conflict Management Styles and Psychological Empowerment among Nursing Students in Clinical Placement: A Structural Equation Modeling Approach
- Liping Ren1, Hyunli Kim2,
-
Journal of Korean Academy of Nursing 2017;47(5):700-711.
DOI: https://doi.org/10.4040/jkan.2017.47.5.700
Published online: January 15, 2017
1College of Nursing, Jining Medical University, Jining, Shandong, China
2College of Nursing, Chungnam National University, Daejeon,
2College of Nursing, Chungnam National University, Daejeon,
-
Corresponding author:
Hyunli Kim,
Email: hlkim@cnu.ac.kr
Received: 10 March 2017 • Revised: 29 August 2017 • Accepted: 31 August 2017
Abstract
This study aimed to test a proposed structural equation model in which bullying experience, conflict management styles and psychological empowerment predict psychological well-being among Chinese nursing students in clinical placement.
Three hundred and sixty-six nursing students recruited from five hospitals in J city and Y city were assessed with self-report questionnaires on bullying experience, conflict management styles, psychological empowerment and psychological well-being including depression, self-esteem, and academic major satisfaction. Data were analyzed using SPSS version 20.0 and AMOS version 22.0.
The evaluation parameters included the comparative fit index at .90, the goodness of fit index at .93, the root mean square error of approximation at .07, and c2/df ratio at 2.66, indicating that the proposed structural equation model provided a good fit to the data. Experience of being bullied during clinical placement, conflict management styles and psychological empowerment explained 93.0% of the variance and had significant effects on psychological well-being, with conflict management styles and psychological empowerment mediating the association between bullying and psychological well-being.
The findings indicated that mediation by conflict management styles and psychological empowerment alleviated the negative influence of bullying on psychological well-being. To limit bullying and its negative effects, development of effective guidelines to deal with bullying will be a critical tool for both Chinese nursing students and their instructors. Further research should incorporate conflict management styles and psychological empowerment into the specific intervention strategies for handling bullying behaviors among nursing students and staff nurses and promoting nursing students’ psychological well-being.
J Korean Acad Nurs. 2017 Oct;47(5):700-711. English.
Published online Oct 31, 2017.
https://doi.org/10.4040/jkan.2017.47.5.700
Published online Oct 31, 2017.
https://doi.org/10.4040/jkan.2017.47.5.700
© 2017 Korean Society of Nursing Science
Original Article
Effects of Bullying Experience on Psychological Well-Being Mediated by Conflict Management Styles and Psychological Empowerment among Nursing Students in Clinical Placement: A Structural Equation Modeling Approach
Liping Ren,1
and Hyunli Kim 2
2
Abstract
Purpose
This study aimed to test a proposed structural equation model in which bullying experience, conflict management styles and psychological empowerment predict psychological well-being among Chinese nursing students in clinical placement.
Methods
Three hundred and sixty-six nursing students recruited from five hospitals in J city and Y city were assessed with self-report questionnaires on bullying experience, conflict management styles, psychological empowerment and psychological well-being including depression, self-esteem, and academic major satisfaction. Data were analyzed using SPSS version 20.0 and AMOS version 22.0.
Results
The evaluation parameters included the comparative fit index at .90, the goodness of fit index at .93, the root mean square error of approximation at .07, and χ2/df ratio at 2.66, indicating that the proposed structural equation model provided a good fit to the data. Experience of being bullied during clinical placement, conflict management styles and psychological empowerment explained 93.0% of the variance and had significant effects on psychological well-being, with conflict management styles and psychological empowerment mediating the association between bullying and psychological well-being.
Conclusion
The findings indicated that mediation by conflict management styles and psychological empowerment alleviated the negative influence of bullying on psychological well-being. To limit bullying and its negative effects, development of effective guidelines to deal with bullying will be a critical tool for both Chinese nursing students and their instructors. Further research should incorporate conflict management styles and psychological empowerment into the specific intervention strategies for handling bullying behaviors among nursing students and staff nurses and promoting nursing students' psychological well-being.
Keywords
Nursing students; Bullying; Depression; Self concept; Personal satisfaction
INTRODUCTION
Nursing shortage is a global issue, more serious in China than in many developed counties [1, 2]. Increasing retention of nursing students is essential for shortage in nursing profession, but about a third of new graduate nurses intend to leave their occupation because of experiencing bullying [3]. Due to a high risk of being bullied in clinical placement, nursing students have low level of psychological well-being and do not able to successfully transform from undergraduate students to new graduate nurses [4, 5]. Appropriate conflict management styles and high level of psychological empowerment are effective methods to help nursing students to reduce detrimental effects of bullying experience [6, 7, 8]. While a growing body of knowledge [4, 9, 10] supports the association of bullying experience with poor psychological outcomes and intention to leave, few studies measured the relationships among bullying experience, conflict management styles, psychological empowerment and psychological well-being in the population of nursing students practicing in hospital. Moreover, it is unclear whether the relationship among bullying experience and psychological well-being is mediated by conflict management styles and psychological empowerment. Given this gap in the literature, the purpose of this research was to test a proposed structural equation model in which bullying experience, conflict management styles and psychological empowerment predict psychological well-being among Chinese nursing students in clinical placement.
Bullying referred as horizontal violence, interpersonal conflict, incivility, mobbing, and intimidation [4, 8, 11]. In this study, bullying was defined as act of aggression or hostility perpetrated deliberately or unconsciously by one person on one or more and can repeatedly occur in covert or overt ways over a period of time, which are all unwanted by the victim, but clearly cause humiliation, offence, and distress, and that may threaten the performance of the healthcare team and/or cause an unpleasant working environment. Nursing students have the highest risk of experiencing bullying from experienced nurses [4, 12, 13]. The prevalence of bullying experience varies across countries, culture, the definition and tool used to measure bullying. Approximately four fifths of nursing students experienced at least one bullying behavior in the past six months in clinical settings [4]. Reem [12] reported that 98.8% of students had experienced bullying from staff nurse and 86.7% of nursing students in Korea [13].
Psychological well-being was defined as a complex of cognitive and affective reactions to life experience, and Ren et al.'s study [4] measured psychological well-being as a combination of self-esteem, depression, and academic major satisfaction, with consideration for special attributes of psychological well-being for nursing students. Bullying experience is strongly correlated to a reduced psychological well-being in student nurses [4, 11]. Bullying experience is considered a stressor that can have potentially serious consequences for the psychological well-being, which is essential to improve the abilities of nursing students to successfully perform clinical training and to continue their career as regisregistered nurses [4, 5, 8].
Conflict management styles was defined as an individual's patterns of behavior predisposition that develop an individual's behaviors and reactions, it is divided into five modes: Competing, Collaborating, Compromising, Avoiding and Accommodating [14]. The evidence for the relationship between bullying experience and conflict management styles has been well substantiated by previous studies [6]. Research has suggested that the perceived bullying behaviors received from staff nurses are positively associated with compromising and avoiding [7, 8]. Psychological well-being could be reduced by compromising [6]. According to Ting-Toomey et al. [15], the consequences of bullying experience can be positive or negative depending on bullying management styles. However, compromise and avoidance are two of the most prevalent conflict management styles for nursing students. In contrast, they do not choose collaboration or competition as their preferred approaches, although these approaches are suggested as effective solutions to unravel interpersonal conflicts [7, 8, 16]. Accordingly, it is possible that nursing students might not have high level psychological well-being, possibly due to inability to cope with frequent bullying.
Psychological empowerment is defined as critical to surviving a work environment that experiences continuous change, and requires employee initiative and innovation [17]. Bullying experience has been found to be negatively related to psychological empowerment [1], psychological empowerment positively related to psychological well-being [18]. Pryjmachuk et al. [1] reported that workplace bullying experience can result in feelings of powerlessness and psychological distress, eventually leading to attrition in nursing programs, nursing students with low psychological empowerment don't believe in their own abilities, and they always focus on their deficiencies rather than strengths in the complex practice environment of healthcare systems [18]. Laschinger et al. [18] suggested that when new graduate nurses' work environments provide access to empowering work structures, their exposure to bullying may be less, and that these conditions promote their health and well-being. However, there has been little research into the relationship between bullying experience, psychological empowerment and psychological well-being.
In China, nurses are paid a very low wage but work extremely long hours doing hard work [2]. A hierarchy, with medicine at the top, developed as hospitals became a major care site, and nursing was dominated by medicine, which benefited hospitals and physicians, but created problems for nursing. Nurses feel alienated and removed from autonomy and control over their working condition, leading to a cycle of low self-esteem and feelings of powerlessness [3]. Instead of fighting back and risking retaliation from superiors, nurses tend to alleviate their own suffering associated with their powerlessness through bullying young coworkers or subordinates [19]. Few Chinese students desire to become a nurse, since most believe they would not gain job satisfaction being a nurse.
A comprehensive model for the primary prevention of bullying and its negative effect on psychological well-being therefore seems necessary to improve understanding in this field. Schlossberg et al.'s transition theory [5] derived theoretical rationale for understanding variables bullying experience, conflict management styles and psychological empowerment that impact the psychological well-being faced by Asian nursing students while interning at hospitals, this theory emphasized on the transitions that bullying experience throughout life and the means by which they cope and adjust. Schlossberg et al. [5] define a transition as “any event or non-event that results in changed relationships, routines, assumptions, and roles about oneself and the world and thus requires a corresponding change in one's behavior”. Transitions exist only if it is defined as experiencing it by the individual. In this study, being bullied can be considered as a transition, and bullying experience was defined as an event that results in changed nursing students' psychological well-being which requires a corresponding change in their intention to leave nursing profession.
Transition may be negative, positive, or neutral, depending on four major factors: situation, self, support, a nd strategies [5], four factors identifying malleable mediators influence the ability of an individual to cope during a transition. Situation described properties of the transition and reflects an individual's perception and appraisal of the transition. Support referred to the people and assets that help a person during a transition. The third factor of self described the demographic and psychological characteristics of individuals, such as individuals' sense of control over their life, being an optimist or pessimist, self-efficacy, commitment, and values. The last factor, strategies, referred to the actions or tactics that individuals use to cope with transition, including having positive beliefs, problem solving, using social skills or using material resources. In this study, psychological empowerment considered as self factor that was defined as psychological characteristics of an individual; conflict management style was strategies, which was defined as actions which an individual used to coping with a transition. Enhancing appropriate conflict management styles and the level of psychological empowerment have been described as essential to preparing nurses for professional nursing practice [6, 7, 8], and the task of measuring mediators of conflict management styles and psychological empowerment that account that account for variation in psychological well-being of interest is the first step in an intervention research model.
Based on obtained empirical evidence from previous studies [1, 6, 7, 8, 18] and Schlossberg et al.'s transition theory [5] (Figure 1), the hypothesized mediation model in the present study proposed that conflict management styles and psychological empowerment mediate the negative effect of bullying experience on psychological well-being in Chinese nursing students. Verification of the relationships among these variables can provide useful knowledge that can be used to build a conceptual framework of bullying experience in Asian nursing students and help nursing students' instructors to develop effective intervention strategies to attain optimal psychological well-being in nursing students' role transition.
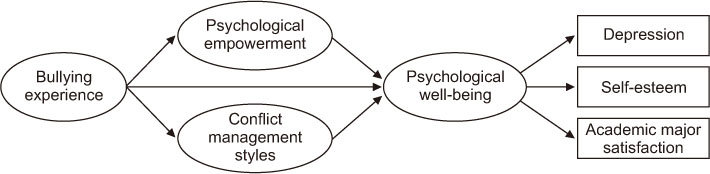
Figure 1
Conceptual framework.
The aims of this study were to identify the relationships among bullying experience, conflict management styles, psychological empowerment and psychological well-being, and to test a proposed model among Chinese nursing students in clinical placement. In addition, the mediation effects of conflict management styles and psychological empowerment between bullying experience and psychological well-being were examined.
METHODS
1. Design
This study was designed as a descriptive, cross-sectional survey to examine the association of bullying experience, conflict management styles, psychological empowerment and psychological well-being especially depression, self-esteem, and academic major satisfaction among students during clinical practice.
2. Participants and data collection
Participants were a convenience sample of 407 nursing students from five hospitals in Y City and J City in China. All participants met the following eligibility criteria: (a) 3rd year students of three-year program (Technical secondary school, Junior college), 4th/5th year students of Undergraduate program in clinical practice for at least six months, (b) students who could speak Chinese language, and (c) nursing students who agreed to participate in the survey with written consent. After their completed questionnaires were sent to the principal investigator, 41 of 407 students were excluded from analysis because of missing data and outliers. The final sample consisted of 366 students. According to Kline [20], an ideal sample size-to-parameters ratio for structural equation modeling analysis would be 20:1, and this research has 15 model parameters, so the ideal sample size is 300. Based on this calculation, the study sample of 366 ensures an adequate number of subjects.
3. Instruments
1) Bullying experience
The short version of the Negative Acts Questionnaire (NAQ) [9] was used to examine nursing students' perception and experiences of bullying in clinic settings. This short version of NAQ was translated into Chinese using a standardized back translation technique with two healthcare professions who were bilingual in Chinese and English. Additional modification was repeated until a consensus within the group for this translation project was reached. To examine the reliability and cultural relevance, a pilot study was conducted with 60 Chinese nursing students who had participated in clinical placement programs for at least six months. Sufficient reliability (Cronbach's α=.86) of this measure was confirmed through this pilot study. Participants were asked how often they had been bullied during their clinical placement. The short version of the NAQ is a five-point Likert scale that scores from 0 never to 4 daily, consisting of 13 items grouped into three factors labeled as follows: Work-related bullying, Person-related bullying, and Physically intimidating bullying. A higher score indicates a higher level of bullying experience. Reliability tested in a previous study was higher than .80 [9], and Cronbach's a coefficient in this study was scored as .86. Cronbach's a coefficient for Work-related bullying was .73, for Person-related bullying was .88, and for Physically intimidating bullying was .87.
2) Conflict management style
The Thomas-Kilmann Conflict Mode Instrument (TKI) was developed from Kilmann & Thomas [14], and was used to identify nursing students' various coping styles. The TKI is a forcedchoice instrument composed of 30 statements pairs, and from each pair the subjects chose one statement to indicate how they would behave during conflict. The instrument included five coping styles: Competing, Collaborating, Compromising, Avoiding and Accommodating. Scores of each of the five coping styles, range from 0 very low use to 12 very high use. Scores of coping styles that fall into the first quartile are considered low use. Similarly, scores that fall into the last quartile are considered high use, and scores that fall into the middle 50 percent are considered medium. TKI had satisfactory test-retest reliability ranged from 0.61 to 0.68 [14]. Despite TKI is an ipsative instrument, traditional alpha reliability cannot be obtained, this instrument has still been proved that carefully designed ipsative tests are useful and valid after all, and have been widely used for occupational assessment [21].
3) Psychological empowerment
Psychological Empowerment Instrument (PEI) was developed from Spreitzer [17], used to reflect an individual's active orientation to his/her work role. It consists of 12 items divided into four subscales: Meaning, Competence, Self-determination and Impact. Each item is rated for frequency and effect on a five-point Likert scale, scored from 1 strongly disagree to 5 strongly agree. The Cronbach's a coefficient of this scale for Meaning was .82, for Competence was .72, for Self-determination was .83, and for Impact was .86 in its development [22]. Cronbach's a coefficient in this study for Meaning was .93, for Competence was .75, for Self-determination was .91, for Impact was .89, and for the total scale was .85.
4) Depression
The Center for Epidemiology Studies-Depression Scale (CESD) was primarily designed for use in studies of the epidemiology of depressive symptomatology in the general population [23]. There are 20 items with a four-point Likert scale, and the response categories for each item ranged from 0 never or rarely to 3 most of the time or all the time. The scores range from 0 to 60, with high scores indicating greater depressive symptoms. The Cronbach's a coefficient of this scale was higher than .80 [23], and Cronbach's a coefficient in this study was .89.
5) Self-esteem
The Self-Esteem Scale (SES) was used to measure a participant's general sense of self-worth and self-acceptance [24]. It consists of 10 statements. Each of the statements scores on a four-point scale from 1 strongly agree to 4 strongly disagree, with composite scores ranging from 10 to 40. A higher score equates to a higher level of self-esteem. Cronbach's a coefficient has been reported higher than .80 [16]. In the current study, Cronbach's α coefficient was .87.
6) Academic major satisfaction
The Academic Major Satisfaction Scale (AMSS) measures nursing students' major field satisfaction [25]. This instrument consists of six items, with a five-point Likert scale ranging from 1 strongly disagree to 5 strongly agree. A higher score represents a student with higher academic major satisfaction. Cronbach's a coefficient was .90 in its development [25], and .73 in this study.
7) General characteristics of participants
General characteristics included gender, age, education program, ethnicity, perceived academic performance, attending bullying management class, receiving any help from teachers or nurses to deal with bullying and relationship between nurses and students.
4. Procedure
At the initial step of this study the authors obtained permission to use the self-report questionnaire instrument from the original developers. After that, the principal investigator contacted potential participants and their instructors to introduce the study and receive their mutual consent. Sufficient information about the purpose, procedure, data confidentiality, and the ethics of withdrawal from study participation were provided, and informed consent was obtained from all students who voluntarily decided to participate in this study. The survey packages including a cover letter, questionnaires, and a small gift were given to them. The principal investigator contacted study participants who did not return questionnaires within one week and encouraged them to send back their questionnaires. Data were collected from January 2014 to February 2014. The return rate was 90.4%.
5. Ethical considerations
This study obtained approval from the Institutional Review Board of the Chungnam National University (IRB approval no. 2013-37). All participants reviewed data confidentiality and survey procedures and voluntarily participated in the study. At the same time, all participants were assured that the questionnaire contents would be used only for research purposes.
6. Data analysis
Data analyses were performed using SPSS version 20.0 and AMOS version 22.0. Prior to initiation of any statistical analyses, accuracy and completeness of all individual data were checked and confirmed. Descriptive statistics were used to characterize study participants. Pearson's correlation coefficients were computed to examine relationships among measured variables. The following assumptions were examined before SEM [20]: missing data, outliers, univariate and multivariate normality, multicollinearity, linearity and homoscedasticity. After deleting outliers, none of the assumptions were violated. Structural Equation Modeling analysis was performed to determine how bullying experience affected psychological well-being through conflict management styles and psychological empowerment. The model fit was assessed by examining the χ2 statistic with a p-value larger than .05, the comparative fit index (CFI), the goodness of fit index (GFI), the root mean square error of approximation (RMSEA), and χ2/df ratio. Significance testing of the total effect, direct effect, and total indirect effects was achieved using the bootstrapping method in AMOS. Baron & Kenny's procedures [26] were used to test the total mediation hypotheses, and significance testing of each mediation effect was achieved using the Sobel test.
RESULTS
1. Sample characteristics
The average age for the sample was 22.00 years (SD=1.79), with a range from 17 to 26 years. Most Chinese nursing students were female, 96.2% of the sample. More than three quarters of the students were of Han nationality (79.5%) and 13.9% was ethnic Korean. About half of the respondents were students of bachelor degree programs. Almost one fifth of the respondents had a low perceived academic performance whereas 32.5% of the participants had a high perceived academic performance. More than half of the students (67.5%) did not attend bullying management class and 43.4% of students did not receive any help from teachers, whereas 68.0% of students did not receive any help from nurses when dealing with bullying experiences. Only 29.0% of students reported that their relationship with nurses was good (see Table 1).
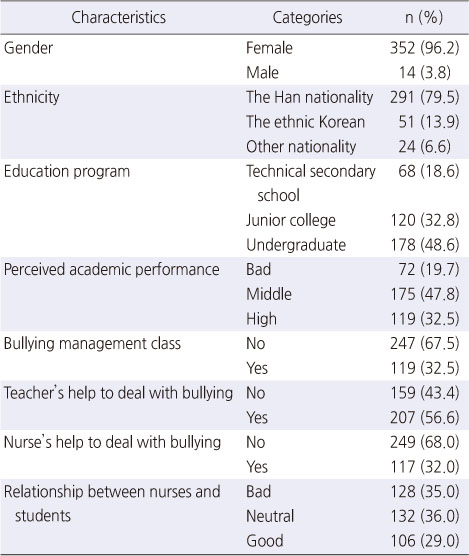
Table 1
Sample Characteristics (N=366)
2. Descriptive statistics and relationships of main variables
Three hundred and fifty-two students (96.1%) reported that they had experienced at least one bullying behavior in the past six months. Avoiding and Compromising were the most frequent style chosen in conflict management, whereas collaborating was the least frequent style. The average score on PEI was 31.01±6.89. The CES-D Score of 16 or higher was considered depressed [23]. In this study, the mean of the CES-D was 22.01 (SD=1.75), indicating a high prevalence (66.7%) of depression in nursing students. The overall score on self-esteem was 20.60± 5.05, and the average score on AMSS was 15.90±4.07.
Of the total sample (407 subjects), 30 cases with more than 5% missing values was deleted from the data set, 35 cases with less than 5% missing values were retained and imputed using the Expectation-Maximization (EM) algorithm [27]. No statistically significant results were found between missing groups and nonmissing groups on other variables. In addition to deleting outliers, standard scores (z) of each item were examined. If |z| >3.00 indicates an outlier, and 11 cases were excluded in this study.
In AMOS, univariate and multivariate normality are evaluated in one step (Table 2). Skewness value's range was -.12~1.56 (absolute skew value <2), and kurtosis value's range was -.07~1.86 (absolute kurtosis value <7), indicating univariate normality of major measured variables. The coefficient of multivariate kurtosis value's associated critical ratio at the bottom of the Table 2 in the row labeled Multivariate was 4.08 (<5) is suggestive of multivariate normality in the sample. Calculating tolerance and Variance inflation factor (VIF) between each variable and all the rest were used to check multicollinearity [20], if tolerance values <.10 or VIF >10.00 may indicate extreme multivariate collinearity. In the present study, there was no evidence of multicollinearity, as the tolerance values ranging from .25 to .80, and VIF ranging from 1.25 to 4.06 (See Table 2). Linearity and homoscedasticity were inspected through the scatterplot matrices. There was no visual evidence of linearity and homoscedasticity being violated.
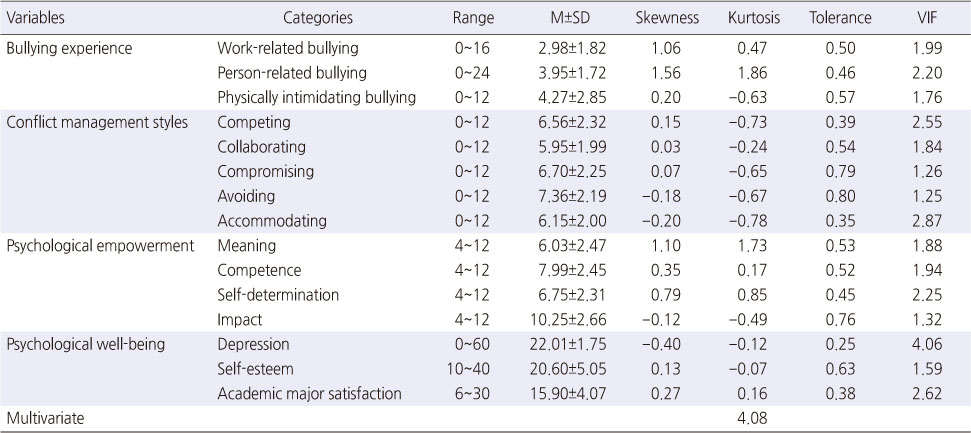
Table 2
Descriptive Statistics of Variables (N =366)
The relationships among the study variables were supported by the correlation analysis, except Self-determination was not correlated with Person-related bullying experience and Physically intimidating bullying experience, and Competing was not correlated with Work-related bullying experience, self-esteem and academic major satisfaction, whereas other types of conflict management styles and the other dimensions of psychological empowerment were significantly associated with bullying experience and psychological well-being. In addition, all the dimensions of bullying experience were significantly correlated with psychological well-being components.
3. Fit indices for the hypothesized model
A hypothesized mediation model was specified with bullying experience as the exogenous variable, conflict management styles and psychological empowerment as the mediators, and psychological well-being as the endogenous variable. The model fit was assessed by examining the χ2 statistic with a p-value larger than .05 indicating failure to reject the null hypothesis. However, the χ2 statistic depends on sample size and data distribution, therefore, the comparative fit index (CFI), the goodness of fit index (GFI), and the root mean square error of approximation (RMSEA) were also used to indicate a good fit [20]. A model is judged to have a good fit if CFI and GFI indices have values higher than .90, and the value of RMSEA is less than .08. The χ2/df ratio is used as a further goodness-of-fit criterion with a χ2/df not larger than 5 [20]. The model fit the data well: χ2=266.13, p=.028, CFI=.90, GFI=.93, RMSEA=.07 and χ2/df=2.66.
4. Model for bullying experience, conflict management styles and psychological empowerment on psychological well-being
In the hypothesized model, bullying experience, conflict management styles and psychological empowerment accounted for 93.0% of the variance in psychological well-being. Standardized regression coefficients (direct, indirect, and total effect) for the hypothesized mediation model are shown in Table 3 and presented in Figure 2. Bullying experience had a significantly positive direct effect on conflict management styles (β=.66, p=.006), a significantly negative direct effect on psychological empowerment (β=-.46, p=.008), and a significantly negative indirect effect on psychological well-being (β=-.69, p=.025). No significant direct for psychological well-being (β=-.01, p=.983) was found. Conflict management styles and psychological empowerment had significant direct effects on psychological well-being, with standardized regression coefficients of -.80 (p=.034) and .36 (p=.009), respectively. Bullying experience, conflict management styles and psychological empowerment in all had a significant negative effect on psychological well-being (bβ=-.68, p=.009).
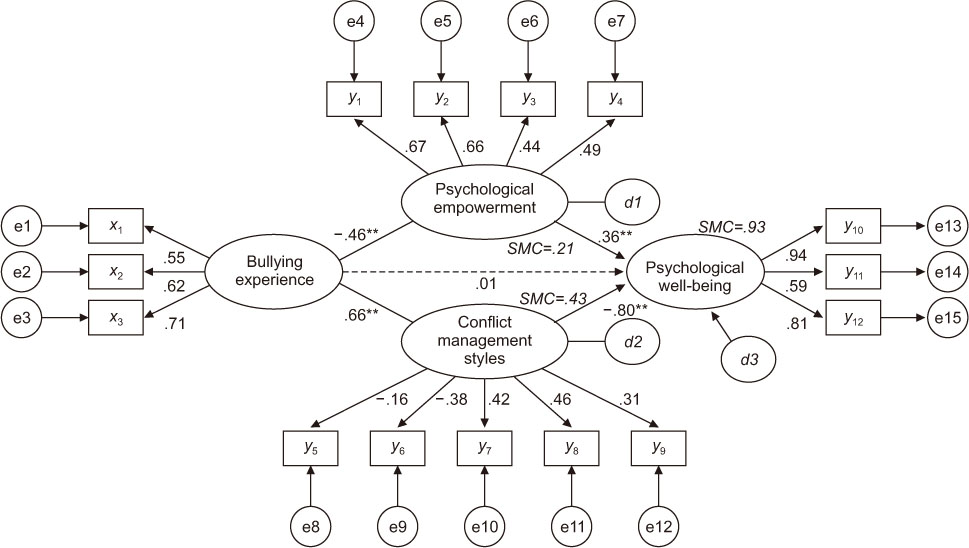
Figure 2
Path diagrams for the hypothetical model

Table 3
Standardized Direct, Indirect, and Total Effects of the Hypothetical Model
5. Effects of conflict management styles and psychological empowerment mediating between bullying experience and psychological well-being
In this study, hypothesis predicts that conflict management styles and psychological empowerment would mediate the relationship between bullying experience and psychological well-being. Thus, four criteria from Baron & Kenny [26] should be met: (a) bullying experience should be significantly associated with psychological well-being; (b) bullying experience should be significantly associated with conflict management styles and psychological empowerment; (c) conflict management styles and psychological empowerment should be significantly associated with psychological well-being; and (d) controlling for conflict management styles and psychological empowerment, the association between bullying experience and psychological well-being should be reduced or no longer significant.
According to Baron & Kenny [26], the first condition was satisfied, the variable of bullying experience was significantly associated with psychological well-being (β=-.66, p=.002). Fulfilling the second condition, the variable of bullying experience was significantly associated with the mediators of conflict management styles and psychological empowerment (Figure 2). The third condition of mediation required that conflict management styles and psychological empowerment were significantly associated with the dependent variable of psychological well-being after controlling for bullying experience (Figure 2). As the fourth condition of mediation required, the effect of bullying experience on psychological well-being was not significant after controlling for the mediators of conflict management styles and psychological empowerment (Figure 2). The direct effect of bullying experience on psychological well-being was -.66 (p=.002), reduced to -.01 (p=.983), confirming the complete mediating role of two mediators. Using the Sobel test was necessary because AMOS provides only the significance of the sum of all indirect effects through multiple mediators and does not allow for testing the significance of each indirect effect. The Sobel test for this mediation model showed a significant mediating effect between bullying experience and psychological well-being: conflict management styles (z=-2.92, p=.003), psychological empowerment (z=-3.56, p<.001). These results indicated that conflict management styles and psychological empowerment completely mediate the effect of bullying experience on psychological well-being, and each single proposed mediator variable showed a significant mediation effect between the relationship of bullying experience and psychological well-being.
DISCUSSION
This study aimed to determine the relationships among bullying experience, conflict management styles, psychological empowerment and psychological well-being for nursing students during clinical placement in China. The results indicated that the proposed model provided a good fit to the data based on the values of various model fit indices, and an adequate structural model of bullying was identified and they support previous studies and enhance our understanding of how bullying experience, conflict management styles and psychological empowerment infiuence psychological well-being. As discussed below, these findings have several theoretical and practical implications.
Regarding the relationship between bullying experience and psychological well-being, the dimensions of bullying experience were found to be positively associated with depression, and negatively associated with self-esteem and academic major satisfaction among nursing students during clinical practice in China. These results are consistent with the results of previous studies [4, 11]. Budden et al. [11] found that the majority of nursing students reported that they experience of being bullied made them feel depressed (53.6%). Even after controlling for general characteristics, nursing students' experience of being bullied was a significant predictor of psychological well-being including depression, self-esteem, and academic major satisfaction [4]. During clinical practice, nursing students described themselves as having a poorly defined and unapproved social role, without a salary, a career, and a stable bond with a specific type of nursing work [28]. Based on the transition theory by Schlossberg et al. [5], bullying as an event may interfere with a successful transition, possibly due to lack of resources to manage stressful situations, and thus fail to integrate new relationships, duties, and roles into daily routines. For this reason, bullying experience could easily undermine nursing students' psychological well-being, which may affect how and whether they will perform their job in the future.
In this study, nursing students preferred avoiding and compromising behaviors to manage conflict, and the conflict management styles had a negative impact on psychological well-being. Previous studies support this finding [7, 8, 16], nursing students scored above the 60th percentile for avoiding [8], and the average score on Compromising was 7.33±2.10 [7]. The choice of inappropriate conflict management styles depends on many variables, such as a mixture of nursing virtue and cultural value toward self-sacrifice [19]. Ni et al. [16] found the mental health of Chinese nursing students was related to the ways of coping, they suggested that avoiding passive coping is very necessary for them to improve the mental health of nursing students. Besides the direct effect of conflict management styles, we also found that bullying experience exerted an indirect effect on psychological well-being through conflict management styles, which was supported by previous studies [6, 29]. Lin et al. [6] reported that although compromising was considered a useful strategy to solving conflict with others for undergraduates, it may also lead to anxiety and depression. Individuals who have inappropriate conflict management styles may be more likely to suffer bullying, compromising interacts with bullying experience at work to predict psychosocial strain [29]. Lack of bullying management skills was not a cause of bullying but a consequence of nursing culture that emphasized self-silencing about bullying as an acceptable way [19]. Preparation in bullying management should start from nursing student education, negative coping styles, such as collaboration or competition [7, 8, 16], were provided through professional guidance can be significant indicators of clinical performance in nursing students and affect the process of role transition from nursing students to staff nurses.
In relation to psychological empowerment and psychological well-being, psychological empowerment had a significant positive impact on psychological well-being, this is consistent with previous studies [10], psychological empowerment increased the academic success among nursing students. In addition, the result showed that bullying experience affect psychological empowerment, which serves as a mitigating factor to reduce effects of bullying experience on psychological well-being [7]. As mentioned before [3, 4], bullying experience and hierarchical structures are pervasive in nursing culture, nursing staff with higher hierarchy feeling superior to unskilled nursing students and engaging in bullying behavior. In China, doctor-patient relationships have been deteriorating for the past 10 years. Medical staffs are involved in tense and confrontational doctor-patient relationships and most patients do not believe medical staff, with even physical attacks on these professionals [28]. In this context, nursing students are not allowed to join fully in clinical practice and may be treated as 'a pair of hands', removed from situations of potentially rich learning. Bradbury-Jones et al. [30] categorized three words for empowerment, which included: 1) leaning in practice (i.e., being understood, encouraged to learn and having responsibility), 2) team membership (i.e., being part of the team), and 3) power (i.e., justice, respect and having a voice). In this study, 43.4% of students did not receive any help from teachers whereas 68.0% of students did not receive any help from nurses when dealing with bullying experiences, and about 71.0% of students reported that their relationship with nurses was not good. Based on these comparisons and the above explanation, it is possible to say that nursing students may frequently encounter absence of continuity of placement, the presence of a mentor and time underpinned empowering experiences, raising problems of low self-esteem, motivation for quitting learning and negative regard for placement [30].
Bullying experience carries with it both short-term and longterm effects on psychological well-being in nursing students. There are psychological responses to the stress from bullying experience dependent on the victims' coping skills and their psychological empowerment level. Bullying experience is harmful to individuals who are bullied constantly and the work environment, unless bullying is monitored and managed. Mediator variables were examined simultaneously, conflict management styles and psychological empowerment received adequate empirical attention, and identifying distinct pathways of influence offer implications for prevention and treatment. These results suggest that more antecedent and mediating variables should be found to explain variance of psychological well-being among nursing students during clinical practice. Using of Schlossberg's Transition Theory may help evaluate relationships of bullying with a wide range of its known correlates in the literature in a more precise way in future research and develop educational intervention to prevent bullying in clinical practice.
CONCLUSION
This study adds significant empirical evidence to the literature on bullying and it will facilitate our understanding of the role of conflict management styles and psychological empowerment in mediating the relationship between bullying experience and psychological well-being in nursing students during clinical placement. The findings of this study suggest that bullying experience is a critical problem among nursing students' psychological well-being including depression, self-esteem and academic major satisfaction. Interventions for increasing nurse psychological well-being should include efforts for reducing bullying experience, improving conflict management styles and providing psychological empowerment. The findings of this study suggest that further research is needed to learn about more mediators between bullying experience and psychological well-being. There is also a need for nursing educators to teach nursing students how to recognize the bullying behaviors. Nursing curriculum is important for nursing students to learn conflict management styles of how to handle bullying behaviors, and practical guidelines are required to promote psychological empowerment in nursing students during clinical training. Furthermore, nurse administrators can utilize these findings to establish policies that create a bully-free culture with supportive and communicative environment in clinical workplace.
Notes
This manuscript is based on a part of the first author's doctoral dissertation from Chungnam National University.
CONFLICTS OF INTEREST:The authors declared no conflict of interest
References
-
Ren L, Kim H, Jung MS. The association between bullying experience related to clinical placement and psychological well-being in nursing students. J Korean Acad Community Health Nurs 2015;26(4):321–329. [doi: 10.12799/jkachn.2015.26.4.321]
-
-
Schlossberg NK, Lynch AQ, Chickering AW. In: Improving higher education environments for adults: Responsive programs and services from entry to departure. San Francisco: Jossey-Bass Inc; 1989. pp. 17.
-
-
Lin WF, Lin YC, Huang CL, Chen LH. We can make it better: “We” moderates the relationship between a compromising style in interpersonal conflict and well-being. J Happiness Stud 2016;17(1):41–57. [doi: 10.1007/Fs10902-014-9582-8]
-
-
Palaz S. Turkish nursing students’ perceptions and experiences of bullying behavior in nursing education. J Nurs Educ Pract 2013;3(1):23–30. [doi: 10.5430/jnep.v3n1p23]
-
-
Budden LM, Birks M, Cant R, Bagley T, Park T. Australian nursing students’ experience of bullying and/or harassment during clinical placement. Collegian 2017;24(2):125–133. [doi: 10.1016/j.colegn.2015.11.004]
-
-
Reem MAER. Paper presented at: Nursing Education Research Conference 2014; 2014 May 13; Indianapolis (IN), USA.
-
-
Park JE. In: Nursing student's experience, their response and coping method of violence [master's thesis]. Busan: Pusan National University; 2013. pp. 1-75.
-
-
Kilmann RH, Thomas KW. Developing a forced-choice measure of conflict-handling behavior: The "Mode" instrument. Educ Psychol Meas 1977;37(2):309–325. [doi: 10.1016/S0147-1767(99)00023-1]
-
-
Ting-Toomey S, Jung KKY, Shapiro RB, Garcia W, Wright TJ, Oetzel JG. Ethnic/cultural identity salience and conflict styles in four US ethnic groups. Int J Intercult Relat 2000;24(1):47–81. [doi: 10.1016/S0147-1767(99)00023-1 ]
-
-
Spreitzer G. Psychological empowerment in the workplace: Dimensions, measurement, and validation. Acad Manage J 1995;38(5):1442–1465. [doi: 10.2307/256865]
-
-
Kline RB. In: Principles and practice of structural equation modeling. New York: The Guilford Press; 2015. pp. 16.
-
-
Li CP, Li XX, Shi K, Chen XF. Psychological empowerment: Measurement and its effect on employee work attitude in China. Xin Li Xue Bao 2006;38(1):99–106.
-
-
Radloff LS. The CES-D scale: A self-report depression scale for research in the general population. Appl Psychol Meas 1977;1(3):385–401. [doi: 10.1177/014662167700100306 ]
-
-
Gray-Little B, Williams VSL, Hancock TD. An item response theory analysis of the Rosenberg self-esteem scale. Pers Soc Psychol Bull 1997;23(5):443–451. [doi: 10.1177/0146167297235001]
-
-
Nauta MM. Assessing college students’ satisfaction with their academic majors. J Career Assess 2007;15(4):446–462. [doi: 10.1177/1069072707305762]
-
-
Greg ACY, Christin M. The psychosocial costs of conflict management styles. Int J Conflict Manage 2010;21(4):382–399. [doi: 10.1108/10444061011079930]
-
 Cite
Cite
