 Submit an article
Submit an article
Articles
- Page Path
- HOME > J Korean Acad Nurs > Volume 42(7); 2012 > Article
-
Original Article
- Multilevel Analysis of Health Care Service Utilization among Medical Aid Beneficiaries in Korea
- Yang Heui Ahn1, Ok Kyung Ham2, Soo Hyun Kim2, Chang Gi Park3
-
Journal of Korean Academy of Nursing 2012;42(7):928-935.
DOI: https://doi.org/10.4040/jkan.2012.42.7.928
Published online: December 12, 2012
1Department of Nursing, Yonsei University Wonju College of Medicine, Wonju, Korea
2Department of Nursing, Inha University, Incheon, Korea
3Office of Global Health Leadership, University of Illinois at Chicago, Illinois, USA
1Department of Nursing, Yonsei University Wonju College of Medicine, Wonju, Korea
2Department of Nursing, Inha University, Incheon, Korea
3Office of Global Health Leadership, University of Illinois at Chicago, Illinois, USA
- Address reprint requests to : Ham, Ok Kyung Department of Nursing, Inha University, Inha-ro 100, Nam-gu, Incheon 402-751, Korea Tel: +82-32-860-8211 Fax: +82-32-874-5880 Email: okkyung@inha.ac.kr, okkyung7@hanmail.net
• Received: May 31, 2012 • Revised: June 18, 2012 • Accepted: November 13, 2012
Copyright © 2012 Korean Society of Nursing Science
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
-
Purpose
- The current study was done to identify individual- and group-level factors associated with health care service utilization among Korean medical aid beneficiaries by applying multilevel modeling.
-
Methods
- Secondary data analysis was performed using data on health care service reimbursement and medical aid case management progress from 15,948 beneficiaries, and data from 229 regions were included in the analysis.
-
Results
- Results of multilevel analysis showed an estimated intraclass correlation coefficient (ICC) of 18.1%, indicating that the group level accounted for 18.1% of the total variance in health care service utilization, and that beneficiaries within the region are more likely to share common features with regard to health care service utilization. At the individual level, existence of disability and types of medical aid beneficiaries showed a significant association, while, at the group level, social deprivation index, and the number of beneficiaries and case managers within the region showed a significant association with health care service utilization.
-
Conclusion
- The significant influence of group level variables in health care service utilization found in this study indicate a need for group level approaches, such as policy change and/ or promotion of community awareness.
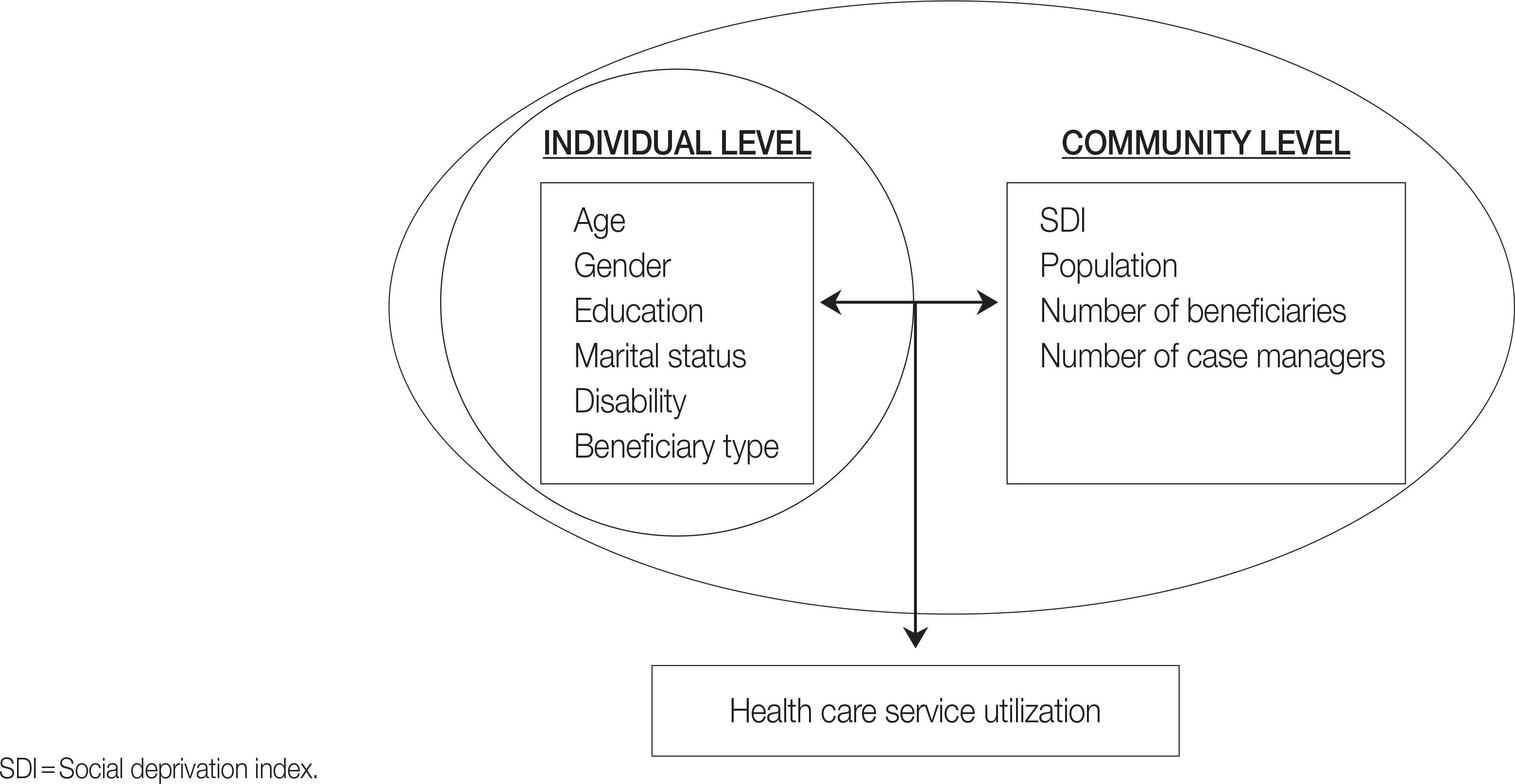
Table 1.General Characteristics of Medical Aid Beneficiaries (N=15,948)
| Individual variable | Distribution | n (%) | M±SD | Range |
|---|---|---|---|---|
| Age (year) | 66.93±12.51 | 11-100 | ||
| Gender | Male | 5,667 (35.5) | ||
| Female | 10,281 (64.5) | |||
| Marital status | Married/cohabitating | 4,460 (28.0) | ||
| Single | 977 (6.1) | |||
| Widowed/divorced/separated | 6,171 (38.7) | |||
| No response | 4,340 (27.2) | |||
| Education (n=19,946) | None | 5,660 (35.5) | ||
| ≤9 years | 6,171 (38.7) | |||
| ≥10 years | 2,243 (14.1) | |||
| No response | 1,874 (11.7) | |||
| Disability | Yes | 6,702 (42.0) | ||
| No | 9,246 (58.0) | |||
| Beneficiary type | Type 1 | 11,255 (70.6) | ||
| Type 2 | 1,737 (10.9) | |||
| Person of national merit | 1,358 (8.5) | |||
| Othera | 1,598 (10.0) | |||
| Health care service utilization (days/6 months) | 1,235.99±585.99 | 1–15,872 | ||
Table 2.Attributes of Group Level Characteristics according to the 229 Regions (N=15,948)
| Group variables | Range | M±SD |
|---|---|---|
| SDI | −1.42-1.69 | −0.10±0.83 |
| Population | 18,221-1,073,149 | 292,585.34±212,291.33 |
| Number of beneficiaries | 468-27,773 | 10,214.73±6,034.24 |
| Number of case managers | 1-10 | 3.40±2.78 |
Table 3.Multilevel Analysis of Health Care Service Utilization according to the 229 Regions (N=15,948)
SDI=Social deprivation index. Variables: Gender 1=male, 2=female; education 1=less than or equal to 9 years, 2=more than 9 years; marriage1=without spouse (single, divorces, widowed, or separated), 2=with spouse; disability 0=not disabled, 1=disabled; beneficiary type 1=type 1, 2=other (type 2, those for persons of national merit, refugees, servicemen, and victims of natural disasters).
- Cho S.H. 2003;Using multilevel analysis in patient and organizational outcomes research. Nursing Research. 52(1):61–65.ArticlePubMed
- Eun S. J., Hong J. Y., Lee J. Y., Lee J. S., Kim Y., Kim Y. I., et al. 2006;Differences in medical care utilization rates of the disabled and the non- disabled with ambulatory care sensitive conditions. Journal of Preventive Medicine and Public Health. 39(5):411–418.PubMed
- Ahn Y. H., Kim E. S., Ham O. K., Kim S. H., Hwang S. S., Chun S. H., et al. 2011;Factors associated with the overuse or underuse of health care services among medical aid beneficiaries in Korea. Journal of Community Health Nursing. 28:190–203. http://dx.doi.org/10.1080/07370016.2011.614837ArticlePubMed
- Bae S. S., Jo H. S., Kim D. H., Choi Y. J., Lee H.J., Lee T. J., et al. 2008;Factors associated with gastric cancer screening of Koreans: Based on a socio-ecological model. Journal of Preventive Medicine & Public Health. 41(2):100–106.Article
- Berben L., Dobbels F., Engberg S., Hill M. N., de Geest, S. 2012;An ecological perspective on medication adherence. Western Journal of Nursing Research. 34(5):635–653. http://dx.doi.org/10.1177/0193945911434518ArticlePubMedPDF
- Chang, Y. 2012.Determinants of gastric cancer screening attendance in Korea: A multi-level analysis. Unpublished master’s thesis. Seoul National University; Seoul.
- Cho S.H. 2003;Using multilevel analysis in patient and organizational outcomes research. Nursing Research. 52(1):61–65.ArticlePubMed
- Eun S. J., Hong J. Y., Lee J. Y., Lee J. S., Kim Y., Kim Y. I., et al. 2006;Differences in medical care utilization rates of the disabled and the non- disabled with ambulatory care sensitive conditions. Journal of Preventive Medicine and Public Health. 39(5):411–418.PubMed
- Hanlon P., Walsh D., Whyte B. W., Scott S. N., Lightbody P., Gilhooly M. L.M. 1998;Hospital use by an ageing cohort: An investigation into the association between biological, behavioural, and social risk markers and subsequent hospital utilization. Journal of Public Health Medicine. 20(4):467–476.ArticlePubMed
- Kim E. Y., Nam E. S., Chae Y. R., Lee H.K. 2008;Factors affecting the elderly’s preference for utilization of long-term care services based on Andersen’s Behavioral Model. Journal of the Korean Gerontological Society. 28(3):585–602.
- Kim S.A. 2012.The effect of case management intervention by medical aid case manager: Centered on medical aid recipients with chronic disease. Unpublished master’s thesis. Hanyang University; Seoul.
- Korea Ministry of Health & Welfare. 2010.2010 medical aid program guide. Seoul: Author.
- Lake E.T. 2006;Multilevel models in health outcomes research part II: Statistical and analytic issues. Applied Nursing Research. 19(2):113–115. http://dx.doi.org/10.1016/j.apnr.2006.01.001ArticlePubMed
- Lee H. J., Oh J. J., Choi J.M. 2010;Comparison of case management between tele care regions and general care regions in Korean Medicaid. Journal of Korean Academy of Nursing Administration. 16(4):381–388.Article
- Lee S.H. 2009;Multi-level analysis of factors related to quality of service in long-term care hospitals. Journal of Korean Academy of Nursing. 39(3):409–421. http://dx.doi.org/10.4040/jkan.2009.39.3.409PubMed
- Lim S.J. 2010;Change in healthcare utilization by disease severity after case management for Medicaid. Journal of Korean Academy of Community Health Nursing. 21(3):321–332.Article
- Medlensky L., Esplen M. J., Gallinger S., McLaughlin J. R., Goel, V. 2003;Relatives of colorectal cancer patients: Factors associated with screening behavior. American Journal of Preventive Medicine. 25(3):187–194. http://dx.doi.org/10.1016/S0749-3797(03)00202-2ArticlePubMed
- Park J. H., Lee J. S., Lee J. Y., Hong J. Y., Kim S. Y., Kim S. O., et al. 2006;Factors affecting national health insurance mass screening participation in the disabled. Journal of Preventive Medicine and Public Health. 39(6):511–519.PubMed
- Park S., Lake E.T. 2005;Multilevel modeling of a clustered continuous outcome. Nursing Research. 54(6):406–413. http://dx.doi.org/10.1097/00006199-200511000-00007ArticlePubMedPMC
- Sallis J. F., Owen N., Fisher E.B. 2008.Ecological models of health behavior. In: Glanz K., Rimer B.K., Viswanath K., editors. Health behavior and health education: theory, research, and practice. 4th ed.San Fransisco: Jossey-Bass.
- Shin S. M., Kim E. S., Park C. K., Lee H.W. 2010a;The medical use of the disabled among overusers of medical aid in Korea. Journal of Preventive Medicine and Public Health. 43(1):35–41. http://dx.doi.org/10.3961/jpmph.2010.43.1.35ArticlePubMed
- Shin S. M., Kim M. J., Kim E. S., Lee H. W., Park C. G., Kim H.K. 2010b;Medical aid service overuse assessed by case managers in Korea. Journal of Advanced Nursing. 66(10):2257–2265. http://dx.doi.org/10.1111/j.1365-2648.2010.05364.xArticlePubMed
- Shin Y. J., Yoon T. H., Kim M. H., Cho H. J., Kim M. K., Yoo W. S., et al. 2009.Health promotion strategies and programs development for health inequalities alleviation. Seoul: Industry-University Cooperation Foundation Hanyang University·Korea Health Promotion Foundation.
- Song M.K. 2011.Factors related to competencies of medical aid case managers. Unpublished master’s thesis. Hanyang University; Seoul.
- Statistics Korea. 2009;Database. Retrieved December 15, 2011, from. http://kostat.go.kr/portal/korea/index.action
- World Health Organization. 2002;World report on violence and health. Retrieved May 16, 2012, from. http://www.emro.who.int/violence-injuries-disabilities/health-topics/
REFERENCES
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
- Exploring the role of social representations in micro-health insurance scheme enrolment and retainment in sub-Saharan Africa: a scoping review
Albino Kalolo, Lara Gautier, Manuela De Allegri
Health Policy and Planning.2022; 37(7): 915. CrossRef - Factors Influencing Emergency Department Nurses’ Compliance with Standard Precautions Using Multilevel Analysis
Su Jung Kim, Eun Ju Lee
International Journal of Environmental Research and Public Health.2021; 18(11): 6149. CrossRef - Factors Affecting Emotional · Behavioral Problems in Early Adolescence: A Multilevel Model Study
Hee Young Park, Yeon Hee Choi
Journal of Korean Academy of Community Health Nursing.2017; 28(4): 482. CrossRef - Equity of access under Korean national long-term care insurance: implications for long-term care reform
Ju Moon Park
International Journal for Equity in Health.2015;[Epub] CrossRef - Ecological Correlates of Cardiovascular Disease Risk in Korean Blue-collar Workers: A Multi-level Study
Won Ju Hwang, Yunhee Park
Journal of Korean Academy of Nursing.2015; 45(6): 857. CrossRef - Prevalence and Predictors of Polypharmacy among Korean Elderly
Hong-Ah Kim, Ju-Young Shin, Mi-Hee Kim, Byung-Joo Park, Terence J. Quinn
PLoS ONE.2014; 9(6): e98043. CrossRef
 Cite
CiteMultilevel Analysis of Health Care Service Utilization among Medical Aid Beneficiaries in Korea
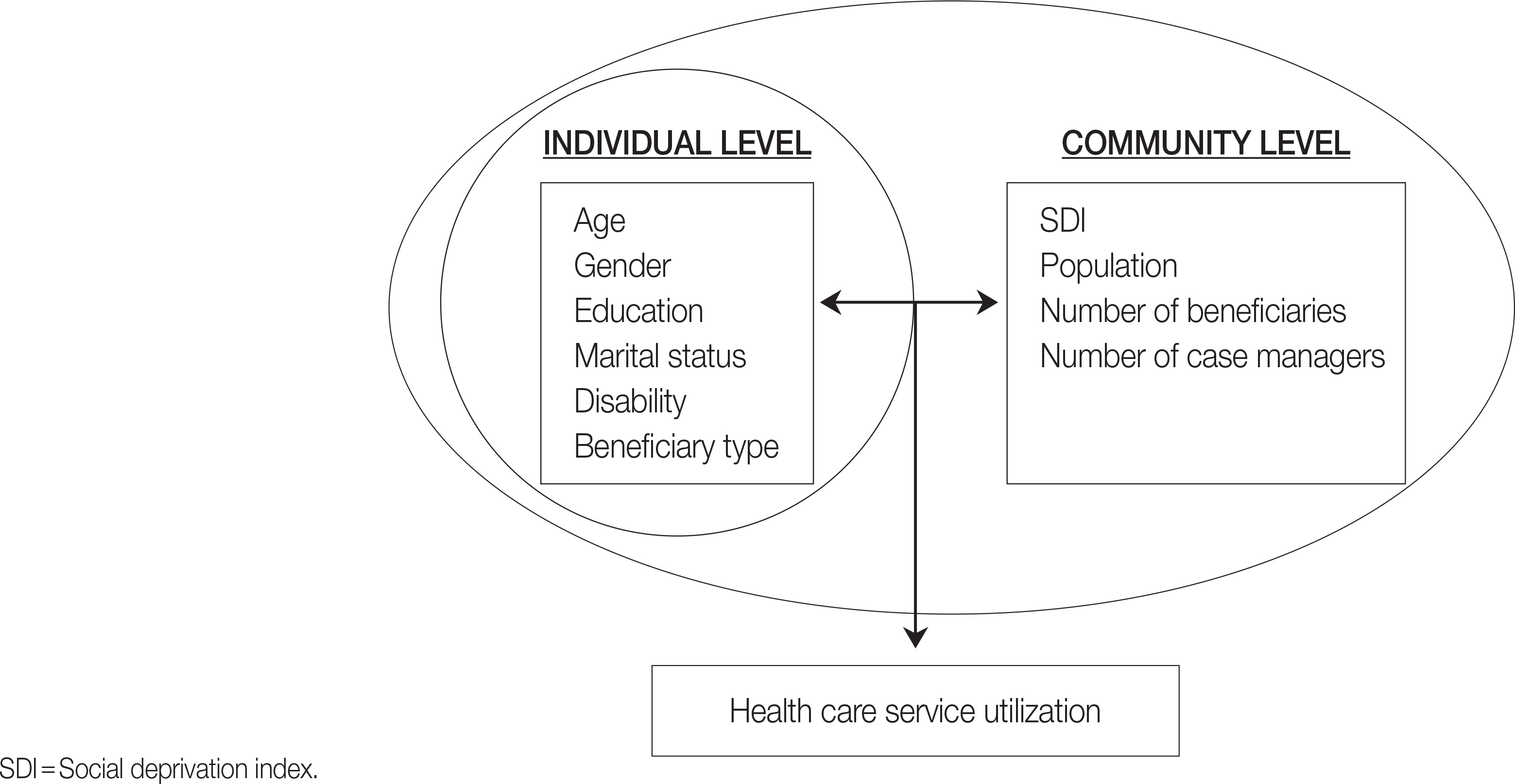
Figure 1. Theoretical framework of the study based on ecological model.
Figure 1.
Multilevel Analysis of Health Care Service Utilization among Medical Aid Beneficiaries in Korea
| Individual variable | Distribution | n (%) | M±SD | Range |
|---|---|---|---|---|
| Age (year) | 66.93±12.51 | 11-100 | ||
| Gender | Male | 5,667 (35.5) | ||
| Female | 10,281 (64.5) | |||
| Marital status | Married/cohabitating | 4,460 (28.0) | ||
| Single | 977 (6.1) | |||
| Widowed/divorced/separated | 6,171 (38.7) | |||
| No response | 4,340 (27.2) | |||
| Education (n=19,946) | None | 5,660 (35.5) | ||
| ≤9 years | 6,171 (38.7) | |||
| ≥10 years | 2,243 (14.1) | |||
| No response | 1,874 (11.7) | |||
| Disability | Yes | 6,702 (42.0) | ||
| No | 9,246 (58.0) | |||
| Beneficiary type | Type 1 | 11,255 (70.6) | ||
| Type 2 | 1,737 (10.9) | |||
| Person of national merit | 1,358 (8.5) | |||
| Other |
1,598 (10.0) | |||
| Health care service utilization (days/6 months) | 1,235.99±585.99 | 1–15,872 | ||
| Group variables | Range | M±SD |
|---|---|---|
| SDI | −1.42-1.69 | −0.10±0.83 |
| Population | 18,221-1,073,149 | 292,585.34±212,291.33 |
| Number of beneficiaries | 468-27,773 | 10,214.73±6,034.24 |
| Number of case managers | 1-10 | 3.40±2.78 |
| Fixed effect | Null model |
Model 1 |
Model 2 |
|||
|---|---|---|---|---|---|---|
| Estimates | p | Estimates | p | Estimates | p | |
| Individual level | ||||||
| Intercept | 1,209.39 | <.001 | 1,325.70 | <.001 | 1,254.37 | <.001 |
| Age | 0.77 | .121 | 0.61 | .258 | ||
| Gender | −1.73 | .890 | −11.42 | .395 | ||
| Education | −27.06 | .099 | −19.12 | .287 | ||
| Marital status | 19.21 | .114 | 15.62 | .232 | ||
| Disability | −28.67 | .014 | −35.98 | .005 | ||
| Beneficiary type | −111.49 | <.001 | −97.17 | <.001 | ||
| Group level | ||||||
| SDI | −73.17 | .044 | ||||
| Population | 0.00 | .678 | ||||
| Number of beneficiaries | 0.02 | .005 | ||||
| Number of case managers | −47.02 | .007 | ||||
| Random effect | Variance component | p | Variance component | p | Variance component | p |
| Residual | 313,859.17 | <.001 | 320,318.59 | <.001 | 285,288.65 | <.001 |
| Intercept (variance) | 69,267.68 | <.001 | 74,194.58 | <.001 | 62,038.82 | <.001 |
| Deviance | 247,649.77 | 165,740.62 | 124,927.58 | |||
| χ2 | 81,909.15 | <.001 | 40,813.04 | <.001 | ||
Table 1. General Characteristics of Medical Aid Beneficiaries (N=15,948)
Included refugees, servicemen, victims of natural disasters etc.
Table 2. Attributes of Group Level Characteristics according to the 229 Regions (N=15,948)
SDI=Social deprivation index.
Table 3. Multilevel Analysis of Health Care Service Utilization according to the 229 Regions (N=15,948)
SDI=Social deprivation index. Variables: Gender 1=male, 2=female; education 1=less than or equal to 9 years, 2=more than 9 years; marriage1=without spouse (single, divorces, widowed, or separated), 2=with spouse; disability 0=not disabled, 1=disabled; beneficiary type 1=type 1, 2=other (type 2, those for persons of national merit, refugees, servicemen, and victims of natural disasters).

