 Submit an article
Submit an article
Articles
- Page Path
- HOME > J Korean Acad Nurs > Volume 46(1); 2016 > Article
-
Original Article
- Development of Korean Intensive Care Delirium Screening Tool (KICDST)
- Ae-Ri-Na Nam, Jee-Won Park
-
Journal of Korean Academy of Nursing 2016;46(1):149-158.
DOI: https://doi.org/10.4040/jkan.2016.46.1.149
Published online: February 29, 2016
1Department of Nursing, Ajou University Medical Center·Nursing Research Institute, Ajou University, Suwon, Korea.
2College of Nursing·Nursing Research Institute, Ajou University, Suwon, Korea.
- Address reprint requests to: Nam, Ae-Ri-Na. Department of Nursing, Ajou Medical Center, 164 Worldcup-ro, Yeongtong-gu, Suwon 16499, Korea. Tel: +82-31-219-4436, Fax: +82-31-219-5520, rina@aumc.ac.kr
• Received: August 8, 2015 • Revised: August 24, 2015 • Accepted: November 12, 2015
© 2016 Korean Society of Nursing Science
This is an Open Access article distributed under the terms of the Creative Commons Attribution NoDerivs License. (http://creativecommons.org/licenses/by-nd/4.0/) If the original work is properly cited and retained without any modification or reproduction, it can be used and re-distributed in any format and medium.
Abstract
-
Purpose
- This study was done to develop of the Korean intensive care delirium screening tool (KICDST).
-
Methods
- The KICDST was developed in 5 steps: Configuration of conceptual frame, development of preliminary tool, pilot study, reliability and validity test, development of final KICDST. Reliability tests were done using degree of agreement between evaluators and internal consistency. For validity tests, CVI (Content Validity Index), ROC (Receiver Operating Characteristics) analysis, known group technique and factor analysis were used.
-
Results
- In the reliability test, the degree of agreement between evaluators showed .80~1.00 and the internal consistency was KR-20=.84. The CVI was .83~1.00. In ROC analysis, the AUC (Area Under the ROC Curve) was .98. Assessment score was 4 points. The values for sensitivity, specificity, correct classification rate, positive predictive value, and negative predictive value were found to be 95.0%, 93.7%, 94.4%, 95.0% and 93.7%, respectively. In the known group technique, the average delirium screening tool score of the non-delirium group was 1.25±0.99 while that of delirium group was 5.07±1.89 (t= - 16.33, p <.001). The factors were classified into 3 factors (cognitive change, symptom fluctuation, psychomotor retardation), which explained 67.4% of total variance.
-
Conclusion
- Findings show that the KICDST has high sensitivity and specificity. Therefore, this screening tool is recommended for early identification of delirium in intensive care patients.
This manuscript is a revision of the first author's doctoral dissertation from Ajou University.
The authors declared no conflict of interest.
- 1. Brown TM, Boyle MF. Delirium. BMJ. 2002;325(7365):644–647. ArticlePubMedPMC
- 2. Devlin JW, Fong JJ, Fraser GL, Riker RR. Delirium assessment in the critically ill. Intensive Care Med. 2007;33(6):929–940. ArticlePubMedPDF
- 3. Ely EW, Inouye SK, Bernard GR, Gordon S, Francis J, May L, et al. Delirium in mechanically ventilated patients: Validity and reliability of the confusion assessment method for the intensive care unit (CAM-ICU). JAMA. 2001;286(21):2703–2710. ArticlePubMed
- 4. Heo EY, Lee BJ, Hahm BJ, Song EH, Lee HA, Yoo CG, et al. Translation and validation of the Korean confusion assessment method for the intensive care unit. BMC Psychiatry. 2011;11:94ArticlePubMedPMCPDF
- 5. van Eijk MM, van Marum RJ, Klijn IA, de Wit N, Kesecioglu J, Slooter AJ. Comparison of delirium assessment tools in a mixed intensive care unit. Crit Care Med. 2009;37(6):1881–1885. ArticlePubMed
- 6. Ely EW, Shintani A, Truman B, Speroff T, Gordon SM, Harrell FE Jr, et al. Delirium as a predictor of mortality in mechanically ventilated patients in the intensive care unit. JAMA. 2004;291(14):1753–1762. ArticlePubMed
- 7. Dubois MJ, Bergeron N, Dumont M, Dial S, Skrobik Y. Delirium in an intensive care unit: A study of risk factors. Intensive Care Med. 2001;27(8):1297–1304. ArticlePubMedPDF
- 8. Suh HJ, Yoo YS. Intensive care unit nurse's knowledge, nursing performance, and stress about delirium. J Korean Acad Adult Nurs. 2007;19(1):55–65.
- 9. Plaschke K, von Haken R, Scholz M, Engelhardt R, Brobeil A, Martin E, et al. Comparison of the confusion assessment method for the intensive care unit (CAM-ICU) with the intensive care delirium screening checklist (ICDSC) for delirium in critical care patients gives high agreement rate(s). Intensive Care Med. 2008;34(3):431–436. ArticlePubMedPDF
- 10. Gaudreau JD, Gagnon P, Harel F, Tremblay A, Roy MA. Fast, systematic, and continuous delirium assessment in hospitalized patients: The nursing delirium screening scale. J Pain Symptom Manage. 2005;29(4):368–375. ArticlePubMed
- 11. Fagundes JA, Tomasi CD, Giombelli VR, Alves SC, de Macedo RC, Topanotti MF, et al. CAM-ICU and ICDSC agreement in medical and surgical ICU patients is influenced by disease severity. PLoS One. 2012;7(11):e51010ArticlePubMedPMC
- 12. Roberts B, Rickard CM, Rajbhandari D, Turner G, Clarke J, Hill D, et al. Multicentre study of delirium in ICU patients using a simple screening tool. Aust Crit Care. 2005;18(1):6–16. ArticlePubMed
- 13. Kim KN, Kim CH, Kim KI, Yoo HJ, Park SY, Park YH. Development and validation of the Korean nursing delirium scale. J Korean Acad Nurs. 2012;42(3):414–423. ArticlePubMed
- 14. Justic M. Does "ICU psychosis" really exist? Crit Care Nurse. 2000;20(3):28–37.ArticlePDF
- 15. Sessler CN, Gosnell MS, Grap MJ, Brophy GM, O'Neal PV, Keane KA, et al. The Richmond agitation-sedation scale: Validity and reliability in adult intensive care unit patients. Am J Respir Crit Care Med. 2002;166(10):1338–1344. ArticlePubMed
- 16. Peterson JF, Pun BT, Dittus RS, Thomason JW, Jackson JC, Shintani AK, et al. Delirium and its motoric subtypes: A study of 614 critically ill patients. J Am Geriatr Soc. 2006;54(3):479–484. ArticlePubMed
- 17. American Psychiatric Association. Diagnostic and statistical manual of mental disorders, fourth edition (DSM-4). Washington, DC: Author; 1994.
- 18. World Health Organization. The tenth revision of the international classification of diseases and related health problems (ICD-10). Geneva, CH: Author; 1992.
- 19. Lynn MR. Determination and quantification of content validity. Nurs Res. 1986;35(6):382–385. ArticlePubMed
- 20. Devlin JW, Marquis F, Riker RR, Robbins T, Garpestad E, Fong JJ, et al. Combined didactic and scenario-based education improves the ability of intensive care unit staff to recognize delirium at the bedside. Crit Care. 2008;12(1):R19ArticlePubMedPMCPDF
- 21. Kwak JH, Kim JB, Choi JS, Kim HC, Jung SW, Lee EJ, et al. Study on standardization of Korean version of psychiatric diagnostic screening questionnaire: The optimal cutoff scores. J Korean Neuropsychiatr Assoc. 2012;51(2):77–84. Article
- 22. Jain G, Chakrabarti S, Kulhara P. Symptoms of delirium: An exploratory factor analytic study among referred patients. Gen Hosp Psychiatry. 2011;33(4):377–385. ArticlePubMed
- 23. Franco JG, Trzepacz PT, Meagher DJ, Kean J, Lee Y, Kim JL, et al. Three core domains of delirium validated using exploratory and confirmatory factor analyses. Psychosomatics. 2013;54(3):227–238. ArticlePubMed
- 24. George C, Nair JS, Ebenezer JA, Gangadharan A, Christudas A, Gnanaseelan LK, et al. Validation of the intensive care delirium screening checklist in nonintubated intensive care unit patients in a resource-poor medical intensive care setting in South India. J Crit Care. 2011;26(2):138–143. ArticlePubMed
- 25. Trzepacz PT. The neuropathogenesis of delirium. A need to focus our research. Psychosomatics. 1994;35(4):374–391. ArticlePubMed
- 26. Ross CA, Peyser CE, Shapiro I, Folstein MF. Delirium: Phenomenologic and etiologic subtypes. Int Psychogeriatr. 1991;3(2):135–147. ArticlePubMed
- 27. Fann JR, Alfano CM, Burington BE, Roth-Roemer S, Katon WJ, Syrjala KL. Clinical presentation of delirium in patients undergoing hematopoietic stem cell transplantation. Cancer. 2005;103(4):810–820. ArticlePubMed
- 28. Morency CR, Levkoff SE, Dick KL. Research considerations. Delirium in hospitalized elders. J Gerontol Nurs. 1994;20(8):24–30. ArticlePubMed
- 29. Yang YH. Comprehension and knowledge about delirium in nurses working at long-term care hospitals or general hospitals. J Korean Acad Soc Nurs Educ. 2010;16(2):312–320. Article
- 30. Stransky M, Schmidt C, Ganslmeier P, Grossmann E, Haneya A, Moritz S, et al. Hypoactive delirium after cardiac surgery as an independent risk factor for prolonged mechanical ventilation. J Cardiothorac Vasc Anesth. 2011;25(6):968–974. ArticlePubMed
REFERENCES
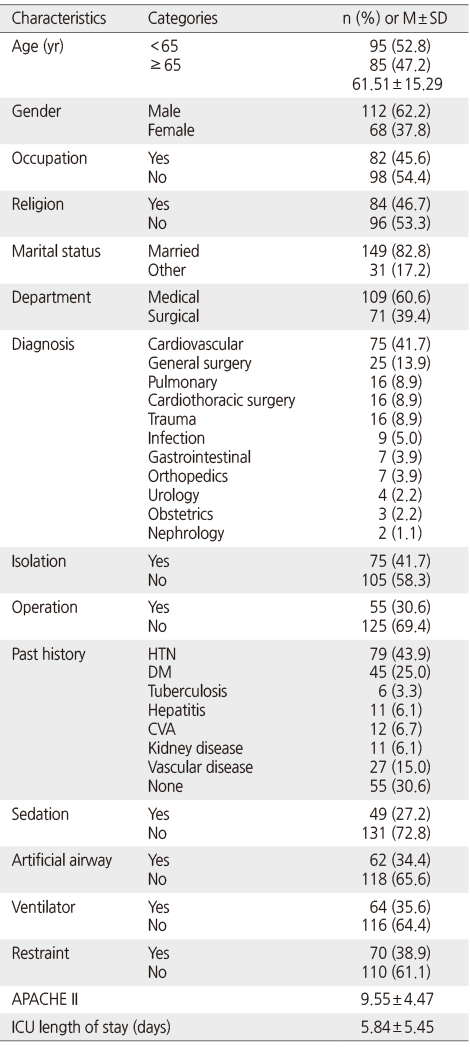
Table 2
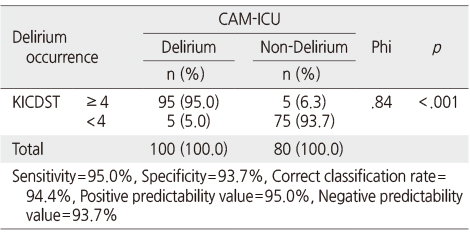
Sensitivity, Specificity, Correct Classification Rate, Predictability Value and Correlation of KICDST with CAM-ICU (N =180)
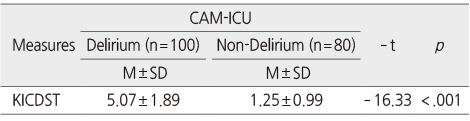
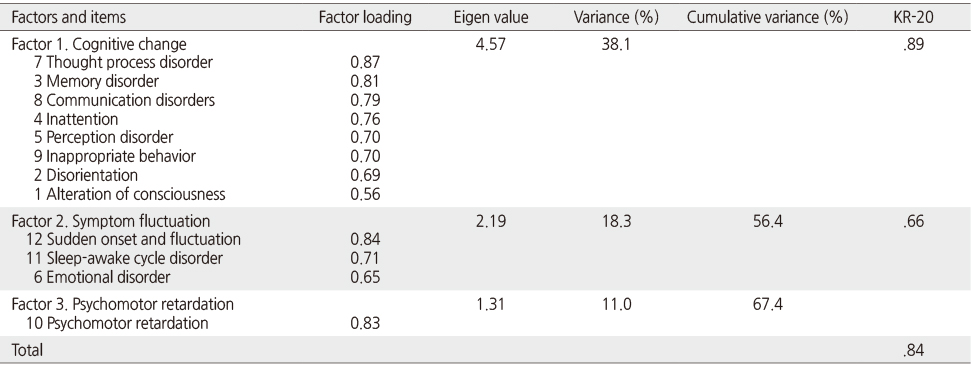
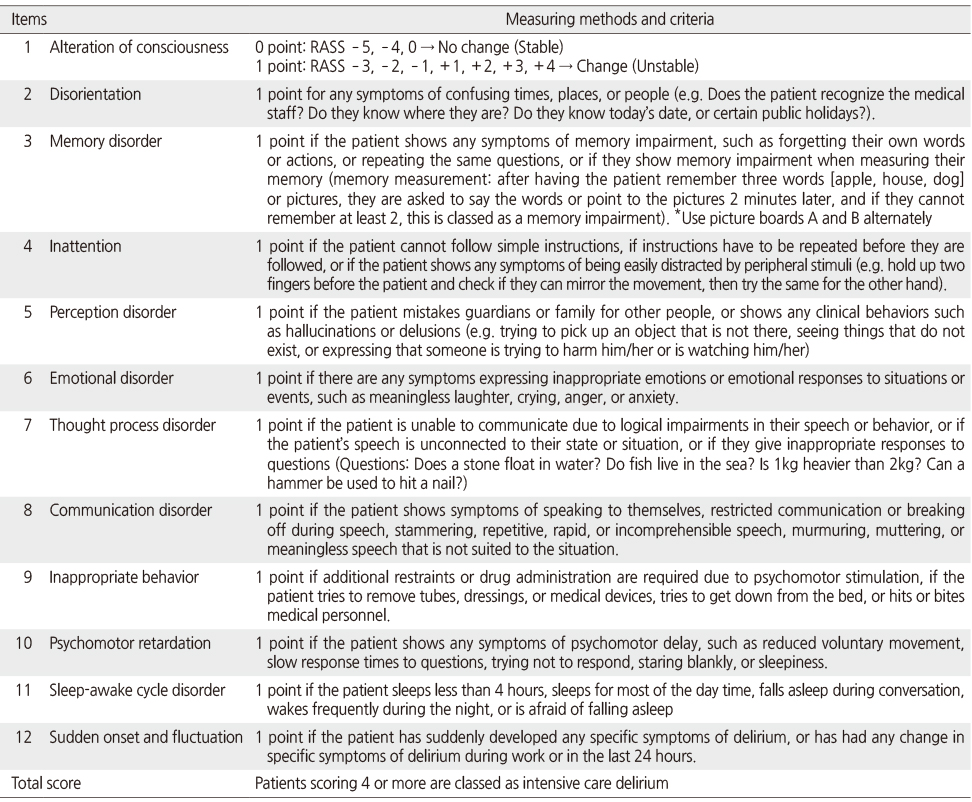
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
- Comparison of the Validity of the PRE-DELIRIC model and the E-PRE-DELIRIC model for Predicting Delirium in patients after Cardiac Surgery
Eun Ju Cho, Myoung Soo Kim
Journal of Korean Academy of Fundamentals of Nursing.2024; 31(3): 275. CrossRef
 Cite
CiteDevelopment of Korean Intensive Care Delirium Screening Tool (KICDST)
Development of Korean Intensive Care Delirium Screening Tool (KICDST)
General and Disease Related Characteristics of the Participants (N =180)
APACHE II=Acute physiologic and chronic health evaluation; ICU=Intensive care unit; HTN=Hypertension; DM=Diabetes mellitus; CVA=Cerebrovascular accident.
Sensitivity, Specificity, Correct Classification Rate, Predictability Value and Correlation of KICDST with CAM-ICU (N =180)
KICDST=Korean Intensive Care Delirium Screening Tool; CAM-ICU=Confusion Assessment Method for the Intensive Care Unit.
Comparison of Delirium Occurrence by KICDST Score (N =180)
KICDST=Korean Intensive Care Delirium Screening Tool; CAM-ICU=Confusion Assessment Method for the Intensive Care Unit.
Factor Analysis of KICDST
Kaiser-Meyer-Olkin test=0.84; Bartlett's test of sphericity p <.001; KICDST=Korean Intensive Care Delirium Screening Tool.
Items and Measuring Methods and Criteria of KICDST
KICDST=Korean Intensive Care Delirium Screening Tool.
Table 1
General and Disease Related Characteristics of the Participants (N =180)
APACHE II=Acute physiologic and chronic health evaluation; ICU=Intensive care unit; HTN=Hypertension; DM=Diabetes mellitus; CVA=Cerebrovascular accident.
Table 2
Sensitivity, Specificity, Correct Classification Rate, Predictability Value and Correlation of KICDST with CAM-ICU (N =180)
KICDST=Korean Intensive Care Delirium Screening Tool; CAM-ICU=Confusion Assessment Method for the Intensive Care Unit.
Table 3
Comparison of Delirium Occurrence by KICDST Score (N =180)
KICDST=Korean Intensive Care Delirium Screening Tool; CAM-ICU=Confusion Assessment Method for the Intensive Care Unit.
Table 4
Factor Analysis of KICDST
Kaiser-Meyer-Olkin test=0.84; Bartlett's test of sphericity
Table 5
Items and Measuring Methods and Criteria of KICDST
KICDST=Korean Intensive Care Delirium Screening Tool.

