 Submit an article
Submit an article
Search
- Page Path
- HOME > Search
Research Paper
- Development of a machine learning-based prediction model for early hospital readmission after kidney transplantation: a retrospective study
- Hye Jin Chong, Ji-hyun Yeom
- J Korean Acad Nurs 2025;55(4):528-542. Published online November 21, 2025
- DOI: https://doi.org/10.4040/jkan.25030
-
 Abstract
Abstract
 PDF
PDF ePub
ePub - Purpose
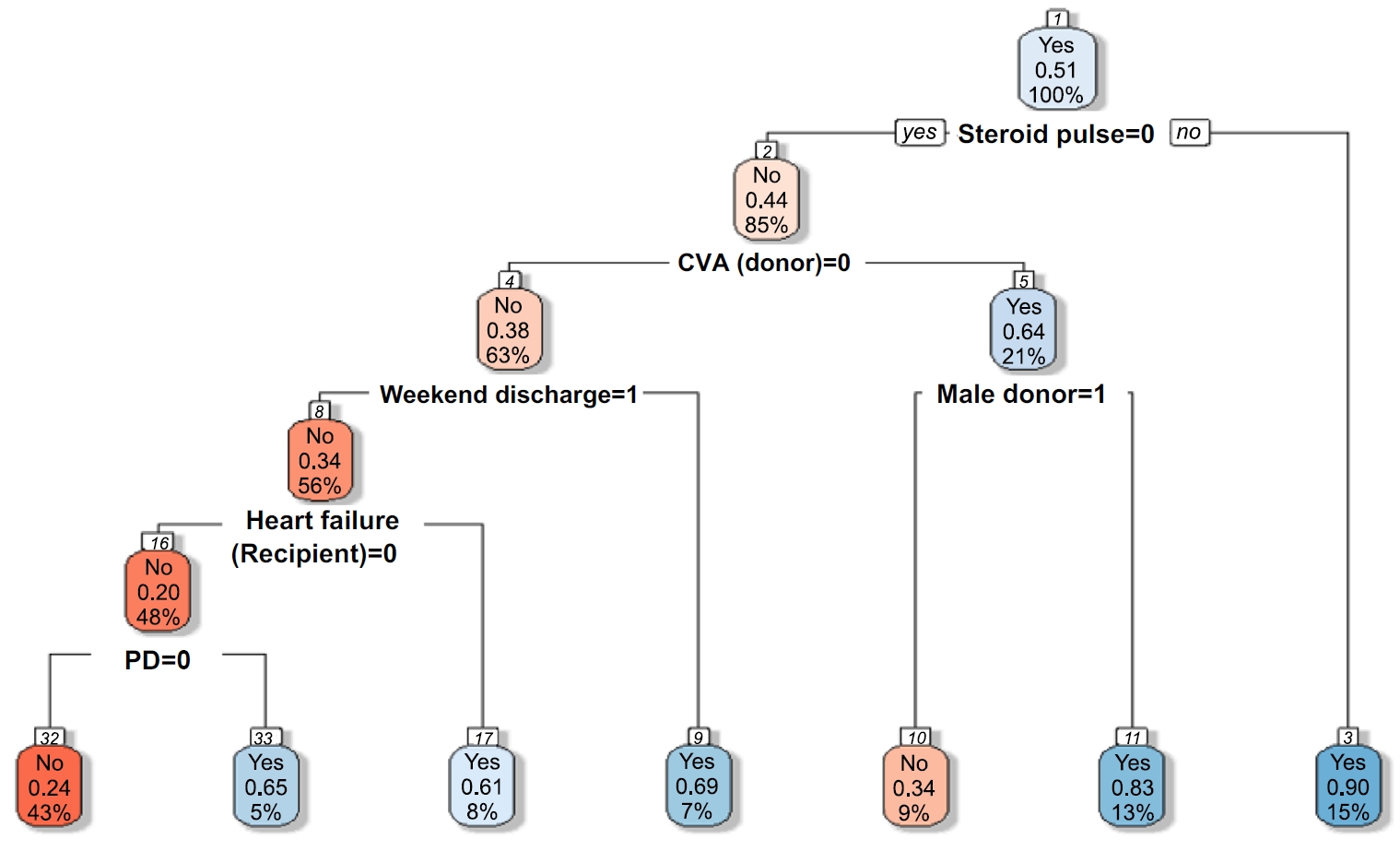
This study aimed to develop and validate a machine learning-based prediction model for early hospital readmission (EHR) post-kidney transplantation.
Methods
The study was conducted at the organ transplantation center of a university hospital, utilizing data from 470 kidney transplant recipients. We built and trained four machine learning models and tested them to identify the strongest EHR predictors. Predictive performance was evaluated using confusion matrices and the area under the receiver operating characteristic curve (ROC AUC).
Results
Among the 470 kidney transplant recipients with a mean age of 46.1 ± 12.02 years, 322 (68.5%) were males, and 74 (15.7%) were readmitted within 30 days after kidney transplantation. In total, 241 (51.2%) recipients were found to have experienced EHR after applying the random over-sampling examples method. The random forest model achieved the best performance, with an ROC AUC of .87 (validation set) and .82 (test set). The 15 most important features were steroid pulse therapy (recipient), cerebrovascular accident (recipient), heart failure (recipient), male sex (donor), cardiovascular disease (recipient), weekend discharge (recipient), peritoneal dialysis (recipient) cerebrovascular accident as the cause of brain death (donor), current smoker (recipient), cardiac arrest (donor), previous kidney transplantation (recipient), age (donor), hypertension (donor), male sex (recipient), and dialysis duration (recipient).
Conclusion
Our framework demonstrated strong predictive interpretability. It can support appropriate and effective clinical decision-making by assisting transplant professionals in stratifying recipients based on their risk of EHR. prioritizing post-discharge care and follow-up for high-risk individuals, and allocating targeted interventions such as closer monitoring or education.
- 2,055 View
- 214 Download

Original Articles
- Reliability and Validity of Korean Version of Nursing Students’ Anxiety and Self-Confidence with Clinical Decision Making Scale
- Mi Yu, Young Eun, KA White, KyungJa Kang
- J Korean Acad Nurs 2019;49(4):411-422. Published online January 15, 2019
- DOI: https://doi.org/10.4040/jkan.2019.49.4.411
-
Abstract
PDF
Abstract Purpose The purpose of this study was to adapt, modify, and validate the Nursing Anxiety and Self-Confidence with Clinical Decision-Making Scale (NASC-CDM©) for Korean nursing students.
Methods Participants were 183 nursing students with clinical practice experience in two nursing colleges. The construct validity and reliability of the final Korean version of the NASC-CDM© were examined using exploratory and confirmatory factor analyses and testing of internal consistency reliability. For adaptation and modification, the instrument was translated from English to Korean. Expert review and a cross-sectional survey were used to test the instrument's validity.
Results The Korean version of the NASC-CDM© (KNASC-CDM) was composed of 23 items divided into four dimensions: (i) Listening fully and using resources to gather information; (ii) Using information to see the big picture; (iii) Knowing and acting; and (iv) Seeking information from clinical instructors. The instrument explained 60.1% of the total variance for self-confidence and 63.1% of the variance for anxiety; Cronbach's α was .93 for self-confidence and .95 for anxiety.
Conclusion The KNASC-CDM can be used to identify anxiety and self-confidence in nursing students’ clinical decision-making in Korea. However, further research should be done to test this instrument, as it is classified differently from the original NASC-CDM© version.
-
Citations
Citations to this article as recorded by
- The Impact of Nursing Students’ Anxiety in Clinical Decision-Making on Relationship-Centered Care: The Mediating Effects of Coherence and Emotional Intelligence
HeeKyung Chang, JinYeong Ahn, MinJi Park, Youngjoo Do
Western Journal of Nursing Research.2026; 48(6): 641. CrossRef - Emergency Nurses' Experiences and Perceptions of Providing Oral Care for Patients
Jung Kuk Bae, Heeje Yun, Eun Bin Lee, Min Jin Choi
Journal of Korean Association for Qualitative Research.2026; 11(1): 19. CrossRef - Development and Evaluation of a “Speak-Up” Program for Patient Safety: A Virtual Reality-Based Intervention for Nursing Students
Jeong Hee Jeong, Mi Jin Kim
Healthcare.2025; 13(22): 2860. CrossRef - Effectiveness of an Integrated Simulation Practicum on Readiness for Practice and Self-Confidence in Clinical Decision-Making among Nursing Students
Hyunseon Jeong, Mijung Cho
Journal of Korea Society for Simulation in Nursing.2025; 13(2): 1. CrossRef - The relationship between clinical decision-making levels and self-efficacy levels of operating room nurses
Sedat Kaya, Gizem Kubat Bakir
Perioperative Care and Operating Room Management.2024; 37: 100416. CrossRef - Clinical decision making: validation of the nursing anxiety and self-confidence with clinical decision making scale (NASC-CDM ©) into Spanish and comparative cross-sectional study in nursing students
Daniel Medel, Tania Cemeli, Krista White, Williams Contreras-Higuera, Maria Jimenez Herrera, Alba Torné-Ruiz, Aïda Bonet, Judith Roca
BMC Nursing.2024;[Epub] CrossRef - Development and Implementation of a Mobile-Integrated Simulation for COVID-19 Nursing Practice: A Randomized Controlled Pretest–Posttest Experimental Design
Sun-Hwa Lee, Jeong-Sil Choi
Healthcare.2024; 12(4): 419. CrossRef - Development and evaluation of a collaborative reflection-based debriefing strategy for simulation-based education using virtual simulations in practical nursing: A randomized controlled trial
Ji-Ah Yun, In-Soon Kang
Nurse Education in Practice.2024; 81: 104170. CrossRef - Constructing a Mixed Simulation With 360° Virtual Reality and a High-Fidelity Simulator
Sun Kyung Kim, Youngho Lee, Younghye Go
CIN: Computers, Informatics, Nursing.2023; 41(8): 569. CrossRef - Path model on decision‐making ability of clinical nurses
Minsook Park, Minkyung Gu, Sohyune Sok
Journal of Clinical Nursing.2023; 32(7-8): 1343. CrossRef - Achieving nursing students' clinical practice hours during the COVID‐19 pandemic: Effects of alternative and nonstandard practicum methods
Min Kyung Song, Ji‐Soo Kim
International Journal of Nursing Practice.2023;[Epub] CrossRef - Factors Related to the Problem-solving Ability of Nursing Students Who Experienced Simulation Training
Ji-Won Han
Journal of Korea Society for Simulation in Nursing.2023; 11(2): 17. CrossRef - A Concept Analysis of Nurses’ Clinical Decision Making: Implications for Korea
Sunyoung Oh, Minkyung Gu, Sohyune Sok
International Journal of Environmental Research and Public Health.2022; 19(6): 3596. CrossRef - The Korean version of the Virtual Patient Learning System Evaluation Tool: Assessment of reliability and validity
Hae Jeong An, Jung Suk Choi, Min Roh, Hyun Mi Cho, Eun Ju Choi
Nurse Education Today.2021; 106: 105093. CrossRef
- The Impact of Nursing Students’ Anxiety in Clinical Decision-Making on Relationship-Centered Care: The Mediating Effects of Coherence and Emotional Intelligence
- 4,010 View
- 165 Download
- 11 Web of Science
- 14 Crossref
- Factors on Decision-Making Participation related to Clinical Experience Difference
- Nan Young Lim, Yeo Jin Yi
- Journal of Korean Academy of Nursing 2004;34(2):270-277. Published online March 28, 2017
- DOI: https://doi.org/10.4040/jkan.2004.34.2.270
-
Abstract
PDF
Purpose The purpose of this study was to investigate the relationship between decision-making factors(theoretical knowledge, expertise, empowerment, intuition) and participation in proportion to nurses's clinical experience.
Method Data was collected by quota sampling from July 10, 2001 to August 22, 2001 from 132 clinical nurses who work for 3 General hospitals. Data was analyzed using SPSSWIN 10.0 with crosstab, ANOVA, and stepwise multiple regression.
Result Expertise(F=34.347, p=.000), empowerment(F=29.316, p=.000), and participation(F=3.276, p=.041) were significantly different among 3 clinical experience groups. Clinical experience correlated with expertise(r=.551, p=.000) and empowerment(r=.492, p=.000), and Decision-making participation also correlated with expertise(r=.351, p=.000) and empowerment(r=.265, p=.002). Decision-making participation is effected by theoretical knowledge(under 3.00yr clinical experience), expertise(3.01-5.00yr), and empowerment(above 5.01yr).
Conclusion These findings indicate that factors(theoretical knowledge, expertise, or empowerment) on decision-making participation varies as nurses's clinical experience differs. Therefore, decision-making needs bilateral agreement between staff nurses and nurse managers rather than the responsibility of one.
-
Citations
Citations to this article as recorded by- Structural Equation Modeling on Clinical Decision Making Ability of Nurses
Min Kyoung Park, Soukyoung Kim
Journal of Korean Academy of Nursing.2019; 49(5): 601. CrossRef - Influence of Internal Marketing Perception, Empowerment, and Job satisfaction on Customer Orientation of Clinical Nurses
Eun-Ah Yi, Yeo-Jin Yi
Korean Journal of Occupational Health Nursing.2012; 21(3): 299. CrossRef - Influence of Job Stress and Empowerment on Clinical Nurses' Performance in Small and Medium Hospitals
Young-Mi Kim, Yeo-Jin Yi
Korean Journal of Occupational Health Nursing.2012; 21(3): 258. CrossRef - Influencing Factors on Service Quality of Care Helpers Working for the Elderly in Long Term Care
Yeo-Jin Yi, Kwang-Hi Park
Korean Journal of Occupational Health Nursing.2012; 21(2): 145. CrossRef - The Effects of Case-Based Learning Using Video on Clinical Decision Making and Learning Motivation in Undergraduate Nursing Students
Moon-Sook Yoo, Jin-Hee Park, Si-Ra Lee
Journal of Korean Academy of Nursing.2010; 40(6): 863. CrossRef
- Structural Equation Modeling on Clinical Decision Making Ability of Nurses
- 1,046 View
- 4 Download
- 5 Crossref
- Development and Evaluation of Shared Medical Decision-Making Scale for End-of-Life Patients in Korea
- Kae Hwa Jo
- J Korean Acad Nurs 2012;42(4):453-465. Published online August 31, 2012
- DOI: https://doi.org/10.4040/jkan.2012.42.4.453
-
Abstract
PDF
Purpose The study was done to develop a shared decision-making scale for end-of-life patients in Korea.
Methods The process included construction of a conceptual framework, generation of initial items, verification of content validity, selection of secondary items, preliminary study, and extraction of final items. The participants were 388 adults who lived in one of 3 Korean metropolitan cities: Seoul, Daegu, or Busan. Item analysis, factor analysis, criterion related validity, and internal consistency were used to analyze the data. Data collection was done from July to October 2011.
Results Thirty-four items were selected for the final scale, and categorized into 7 factors explaining 61.9% of the total variance. The factors were labeled as sharing information (9 items), constructing system (7 items), explanation as a duty (5 items), autonomy (4 items), capturing time (3 items), participation of family (3 items), and human respect (3 items). The scores for the scale were significantly correlated among shared decision-making scale, terminating life support scale, and dignified dying scale. Cronbach's alpha coefficient for the 34 items was .94.
Conclusion The above findings indicate that the shared decision-making scale has a good validity and reliability when used for end-of-life patients in Korea.
-
Citations
Citations to this article as recorded by- Factors Associated With End‐of‐Life Care Competencies Among Nurses in Departments With a High Incidence of End‐of‐Life Cases: A Mixed‐Methods Study
So Hyeon Yeon, Kyung Im Kang, Justin Fontenot
Journal of Nursing Management.2026;[Epub] CrossRef - The effect of illness uncertainty and self‐efficacy on the perception of shared decision‐making among parents of infants in the neonatal intensive care unit
Dahae Choi, Hyewon Shin
Nursing in Critical Care.2025;[Epub] CrossRef - Factors influencing the perception of shared decision-making among parents of children with type 1 diabetes mellitus: A cross-sectional study guided by the Ottawa Decision Support Framework
In Hyeong Choi, In Young Cho
Journal of Pediatric Nursing.2025; 85: 346. CrossRef - Shared Decision-Making in Korean Healthcare: A Scoping Review
Yelim Kwon, Seungmin Nam, Soan Shin, Yoong Cho, Jihyun Yoon, Sang-Ho Yoo
Journal of Korean Medical Science.2025;[Epub] CrossRef - Influences of Nursing Professionalism, Empathy, and Clinical Decision-Making Ability on Shared Decision-Making Awareness among Hemodialysis Nurses
Junghwa Yun, Mihyeon Seong, Youngmi Cho, Sohyune Sok, Majed Alamri
Journal of Nursing Management.2024; 2024: 1. CrossRef - An exploratory study on the shared decision-making as a two-way symmetrical communication process : focusing on the communication of kidney dialysis patients
Soojin Kim, Soontae An, Sejoong Kim, Dong-Ryeol Ryu, Hwanhee Kim
Korean Journal of Journalism & Communication Studies.2021; 65(2): 162. CrossRef - Awareness of Doctors’ Shared Decision-Making in Life-Sustaining Care Decisions
Dalyong Kim, Hyun Jung Lee, Soo-Young Yu, Jung Hye Kwon, Hee Kyung Ahn, Jee Hyun Kim, Seyoung Seo, Chi Hoon Maeng, Seungtaek Lim, Do Yeun Kim, Sung Joon Shin
The Korean Journal of Hospice and Palliative Care.2021; 24(4): 204. CrossRef - The Perceptions and Needs of Hospice Palliative Care and Shared Decision Making among Middle-Aged Adults
Na-Yeon Lee, Seungjin Lee, Soo-Kyoung Lee
The Korean Journal of Hospice and Palliative Care.2016; 19(4): 310. CrossRef - Health Care Professional Factors Influencing Shared Medical Decision Making in Korea
Kae-Hwa Jo, Gyeong-Ju An, Hong Seon Lee
Sage Open.2015;[Epub] CrossRef - Effects of an educational programme on shared decision‐making among Korean nurses
Kae‐Hwa Jo, Gyeong‐Ju An
International Journal of Nursing Practice.2015; 21(6): 839. CrossRef - Types of Shared Medical Decision Making for Terminally Ill Patients
Kae Hwa Jo, Gyun Moo Kim
The Korean Journal of Hospice and Palliative Care.2014; 17(4): 278. CrossRef - Factors Affecting Shared Decision Making at End of Life in Korean Adults
Jo Kae-Hwa, An Gyeong-Ju
Holistic Nursing Practice.2013; 27(6): 329. CrossRef - The Impact of Nurses’ Attitude toward Dignified Death and Moral Sensitivity on Their End-of-Life Care Performance
Kae Hwa Jo, Yeon Ja Kim
The Korean Journal of Hospice and Palliative Care.2013; 16(4): 223. CrossRef - Preferences for Care near the End of Life according to Chronic Patients' Characteristics
Seonyoung Yun, Jiyeon Kang
Korean Journal of Adult Nursing.2013; 25(2): 207. CrossRef
- Factors Associated With End‐of‐Life Care Competencies Among Nurses in Departments With a High Incidence of End‐of‐Life Cases: A Mixed‐Methods Study
- 1,904 View
- 28 Download
- 14 Crossref
 First
First Prev
Prev

